Three different time frames, three different fronts. We continue to muddle through, with some hope that this could be successful relative to our modest expectations.
There’s the situation short term, there’s the new strains, there’s the vaccines.
On the short term front, forward looking news continues to improve, but not at the pace we’d like or that I expected, and the death rate this week unexpectedly (unexpected to me in any case) rose. All signs still point to steady improvement until the new strains have an impact, probably at a pace of something like 1% a day. Hospitalizations aren’t listed in the numbers, but they too are falling steadily.
On the new strain front, the news is mixed.
For the non-English new strains, things got less scary, as it looks much less likely that the new strains can escape and reinfect, or that the vaccines won’t work on them. If they did escape, we learned that the system isn’t capable of responding as quickly as we’d like, but perhaps under duress that would change.
For the English strain, things got much scarier. Previously, we had no reason to think the new strain was more virulent, and if anything were hoping it was less so. Instead, it looks like it’s plausibly substantially more virulent, with 30%+ higher death rates per infection. Given that this strain is about to take over, that’s very bad news.
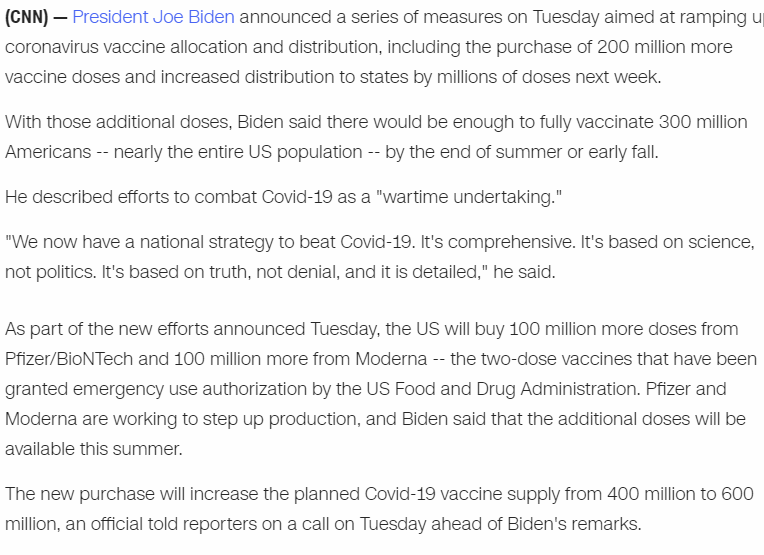
On the vaccine and policy front, we had excellent news, as the Biden administration announced a deal for an additional 200 million doses of vaccine from Pfizer and Moderna.
There’s still a ton to do. We need to approve AstraZeneca now and Johnson & Johnson the moment they release their data. We still need to spend massively to expand capacity. We still need to move to half doses or smaller where available, and legalize rapid testing for real, and so on and so forth. But compared to expectations, I’ll definitely take it.
I’ll also take the numbers we are seeing on vaccinations. They’re not what I wanted to see when this all started, but given how things went until this week, seeing the numbers rise to 1.2 million USA shots a day, with the constraint increasingly being supply, indicates that we’ve mostly muddled through.
The exception to that is our failure in long term care facilities, which isn’t getting enough focus.
Let’s run the numbers.
The Numbers
Predictions
Last week: 11.9% positive rate on 11.3 million tests, and an average of 3,043 deaths.
Prediction: 10.5% positive rate and 2,900 deaths per day.
Result: 11.2% positive rate and 3,257 death per day.
I overshot the drop in positive rate by a factor of two, and the deaths went up rather than slightly down, so not my best prediction week, and poor news all around.
Part of the story about deaths is that our nursing home vaccination efforts have been dreadfully awful, and while I knew they were bad I didn’t appreciate how bad they were. See later on for further discussion. Also I somehow keep not giving holidays proper respect. Presumably this has a lot to do with some combination of Martin Luther King Day, and the continued fallout from New Year’s and Christmas, including secondary little waves as people returned home.
We do see some suggestions in the regional positive test percentages that things might not have started improving until the week of 1/13 in some places, in which case we could still see one more week of things getting worse before they get better. That’s not what I expect, but on looking closer it wouldn’t be that surprising. Once we get deeper into February a lack of improvement would be very surprising.
The other explanation is if the new English strain is much more present than we realize even now, and that it is more virulent than the old strain. I don’t think this impact will be felt for another month or two.
Prediction for next week: 10.8% positive rate, as improvement is clearly ongoing but seems to be slowing down. 3,100 deaths per day, as I still expect this to start dropping, but I can see the case for it taking a bit longer.
Deaths

| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Nov 26-Dec 2 | 1628 | 3814 | 2742 | 1939 |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
| Dec 10-Dec 16 | 3278 | 5324 | 4376 | 3541 |
| Dec 17-Dec 23 | 3826 | 5158 | 5131 | 3772 |
| Dec 24-Dec 30 | 3363 | 3668 | 4171 | 3640 |
| Dec 31-Jan 6 | 4553 | 4127 | 5019 | 4162 |
| Jan 7-Jan 13 | 6280 | 3963 | 7383 | 4752 |
| Jan 14-Jan 20 | 5249 | 3386 | 7207 | 4370 |
| Jan 21-Jan 27 | 6281 | 3217 | 8151 | 4222 |
Both the South and West had substantially more deaths this week. The question remains why, and whether this is a data artifact and deaths from last week got shifted to this week, although it’s hard for that to explain the South. This should be the local peak, but it’s possible we have another week to go if we judge by local positive test percentages.
Positive Test Percentages
This section is unavailable right now because my parser that creates the graph stopped giving me non-zero numbers for a number of states, after running it twice. I’ve been ignoring that problem for Hawaii alone, but now it’s a lot more than Hawaii. I don’t want to delay the post longer. Hopefully I can figure out what’s wrong in time for next week.
In the short term, positive test counts adjusted for overall test count should give a close enough answer for our purposes, but longer term I’ll need to fix the parser. If I run into trouble I’ll ask for help.
Positive Tests

| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Dec 10-Dec 16 | 415,220 | 315,304 | 406,353 | 260,863 |
| Dec 17-Dec 23 | 439,493 | 271,825 | 419,230 | 236,264 |
| Dec 24-Dec 30 | 372,095 | 206,671 | 373,086 | 225,476 |
| Dec 31-Jan 6 | 428,407 | 251,443 | 494,090 | 267,350 |
| Jan 7-Jan 13 | 474,002 | 262,520 | 531,046 | 306,604 |
| Jan 14-Jan 20 | 360,874 | 185,412 | 452,092 | 250,439 |
| Jan 21-Jan 27 | 260,180 | 158,737 | 386,725 | 219,817 |
Test counts did drop a bit, but this is what we were hoping this graph would look like, with large drops across all regions.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Dec 3-Dec 9 | 10,466,204 | 13.9% | 1,411,142 | 4.9% | 4.67% |
| Dec 10-Dec 16 | 10,695,115 | 13.9% | 1,444,725 | 4.9% | 5.12% |
| Dec 17-Dec 23 | 10,714,411 | 13.7% | 1,440,770 | 5.1% | 5.57% |
| Dec 24-Dec 30 | 9,089,799 | 13.8% | 1,303,286 | 6.0% | 5.95% |
| Dec 31-Jan 6 | 9,334,345 | 16.4% | 1,365,473 | 7.3% | 6.42% |
| Jan 7-Jan 13 | 11,084,291 | 15.2% | 1,697,034 | 6.6% | 6.93% |
| Jan 14-Jan 20 | 11,300,725 | 11.9% | 1,721,440 | 5.9% | 7.35% |
| Jan 21-Jan 27 | 10,021,716 | 11.2% | 1,679,399 | 5.3% | 7.69% |
I have no explanation for why we did less testing this week than we did the previous week, and did so everywhere including New York. I do not think it was because less people needed tests.
Covid Machine Learning Project
These can be hard to read, I recommend checking the original source.
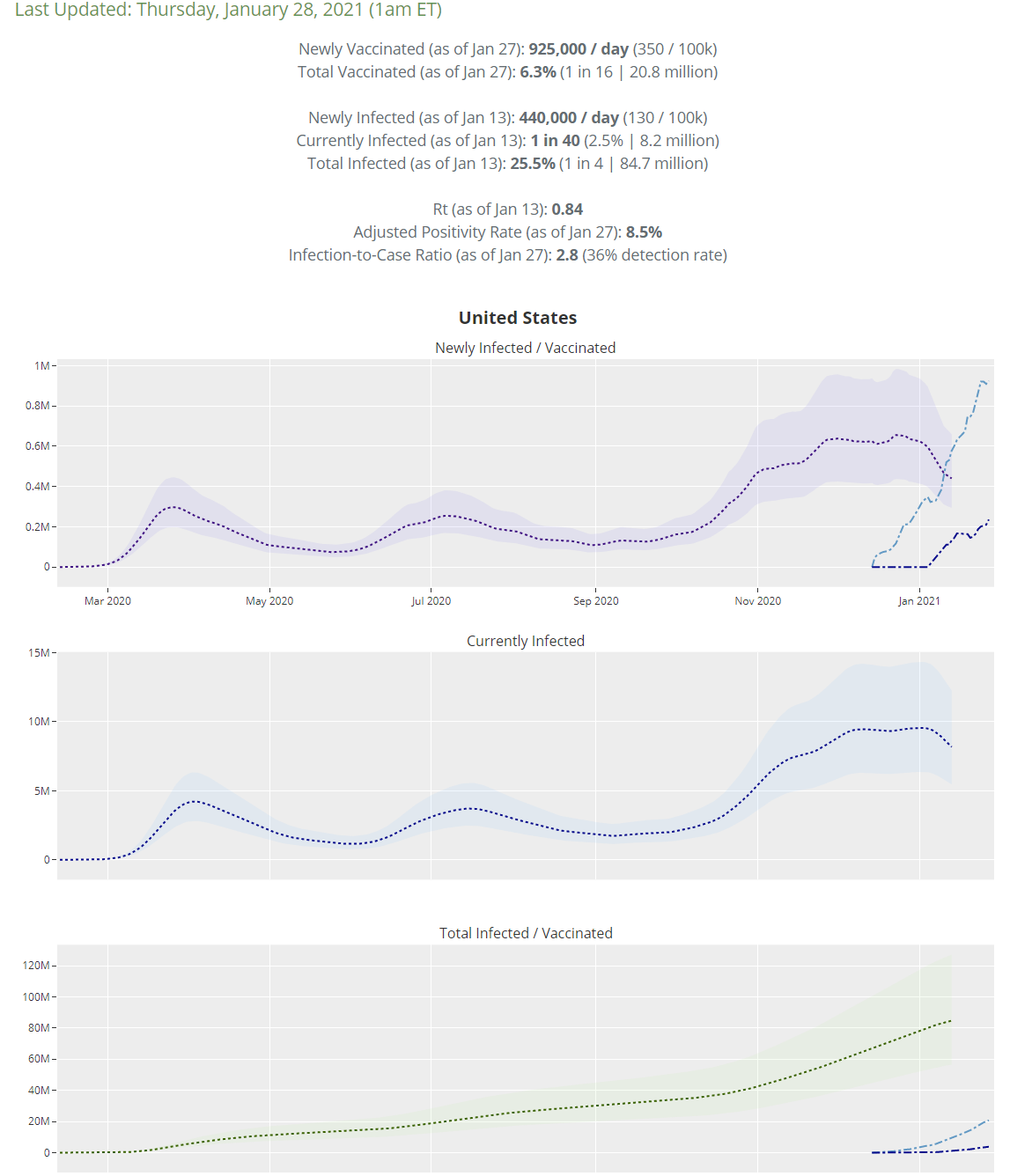
Overall this is a great situation. These projections think R0 is down to 0.84 with the number of infected per day down a third and falling fast.
I’m still the kind of person who is horrified by that tiny little dip in vaccinations in the upper right corner that happened yesterday. It’s expected that this is only a blip, but I’ll feel a lot more comfortable with it in the rear view mirror.
On January 13 they project 25.5% of all Americans as having been infected, up from 24.5% on January 6. That’s still a big compounding edge going forward, which hopefully will rapidly be eclipsed by rising vaccinations.
Vaccinations
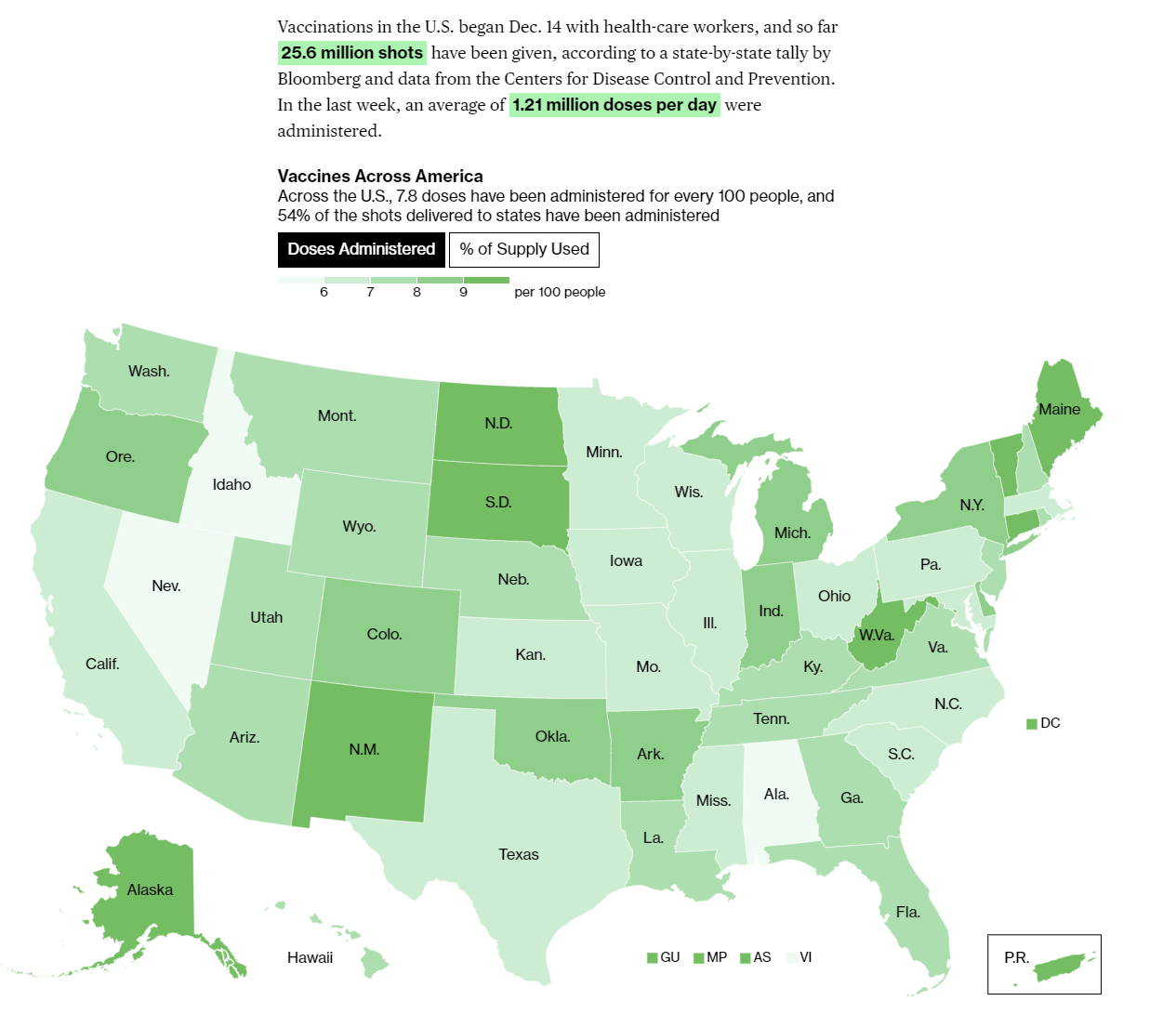
Last week we were averaging under a million doses, now we’re over 1.2 million. That’s a solid rate of increase if it can be sustained. Yesterday saw the seven day average decline slightly, which is always scary, and likely reflects that many states previously were bottlenecked on distribution but are now bottlenecked on supply. So in its own way it is good news, depending on what prior knowledge is being controlled for.
The only questions now are how rapidly we can increase supply, and whether we can use that supply more efficiently.
Europe
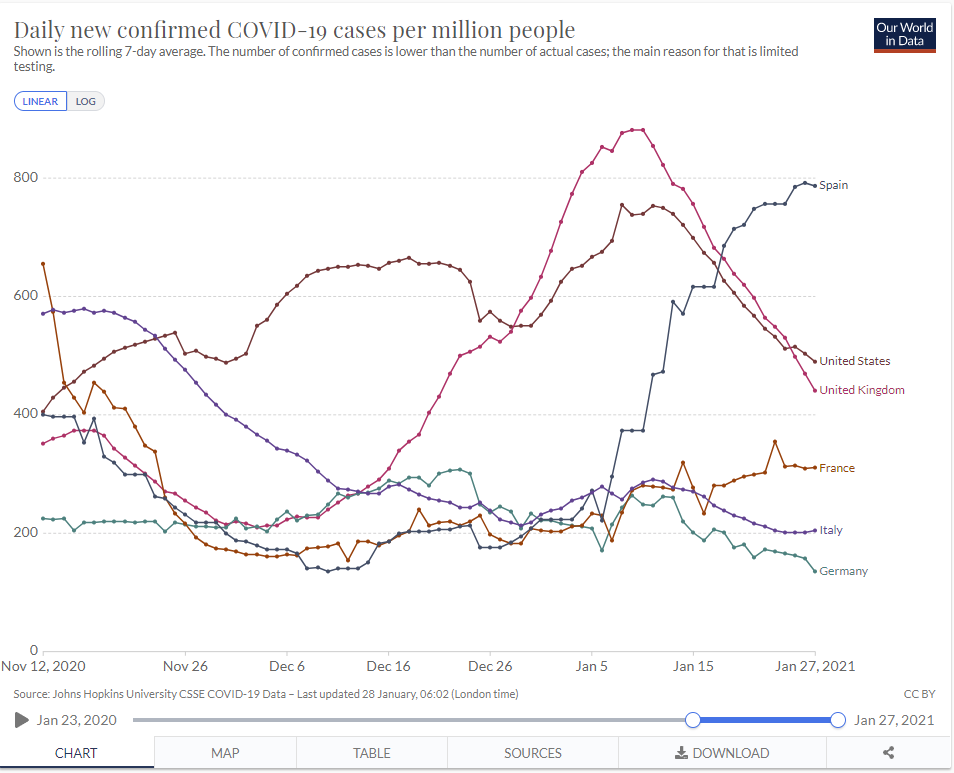
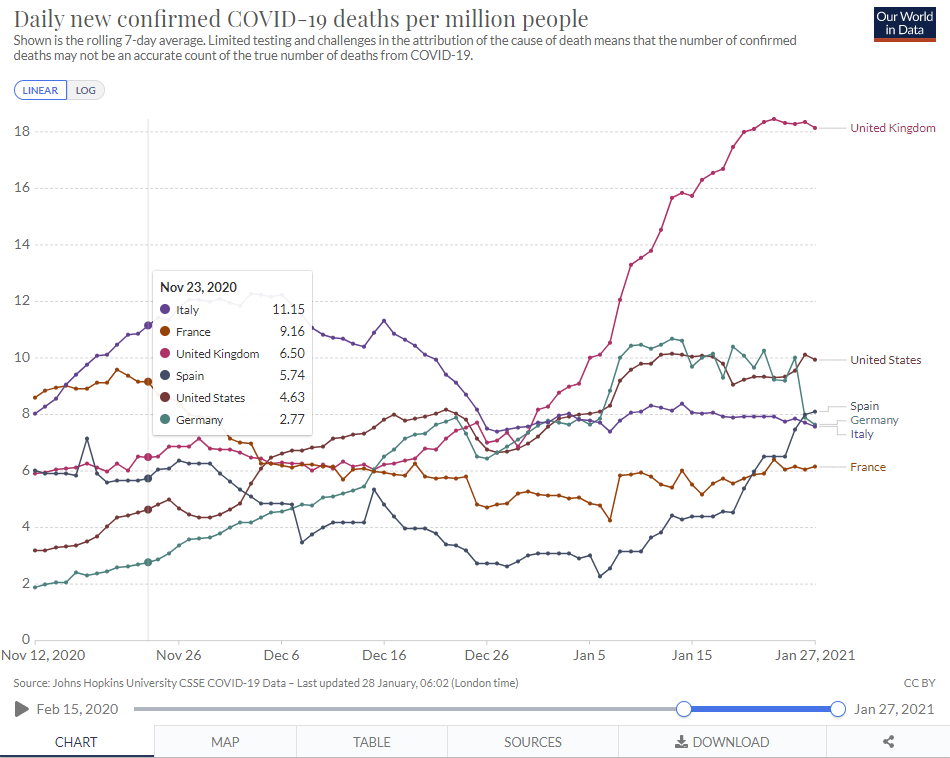
UK positive tests didn’t peak until January 5, so it makes sense that their death counts are only peaking now, but this is still suggestive that the new strain might be more virulent, as will be discussed in the next section. Spain now is approaching the English peak, so we should expect a lot more deaths there starting next week.
The good news is that the UK seems to have things under control, and the lockdown continues to be working. That doesn’t mean they can sustain that level of restrictions, or what the price will be for doing so, but it can definitely be done. I’m not shocked, but I’m definitely pleasantly surprised. I still don’t know if we could do the same, but by the time we need to, we’ll have a lot more help from the already immune.
The English Strain
It is now accepted that the English strain is here, it is rapidly taking over, and it is substantially more infectious than our previous strains.
We know it does not evade vaccines, and prior immunity protects against it. The new worry is that the new strain might be deadlier.

The concerning document everyone’s referring to is here.
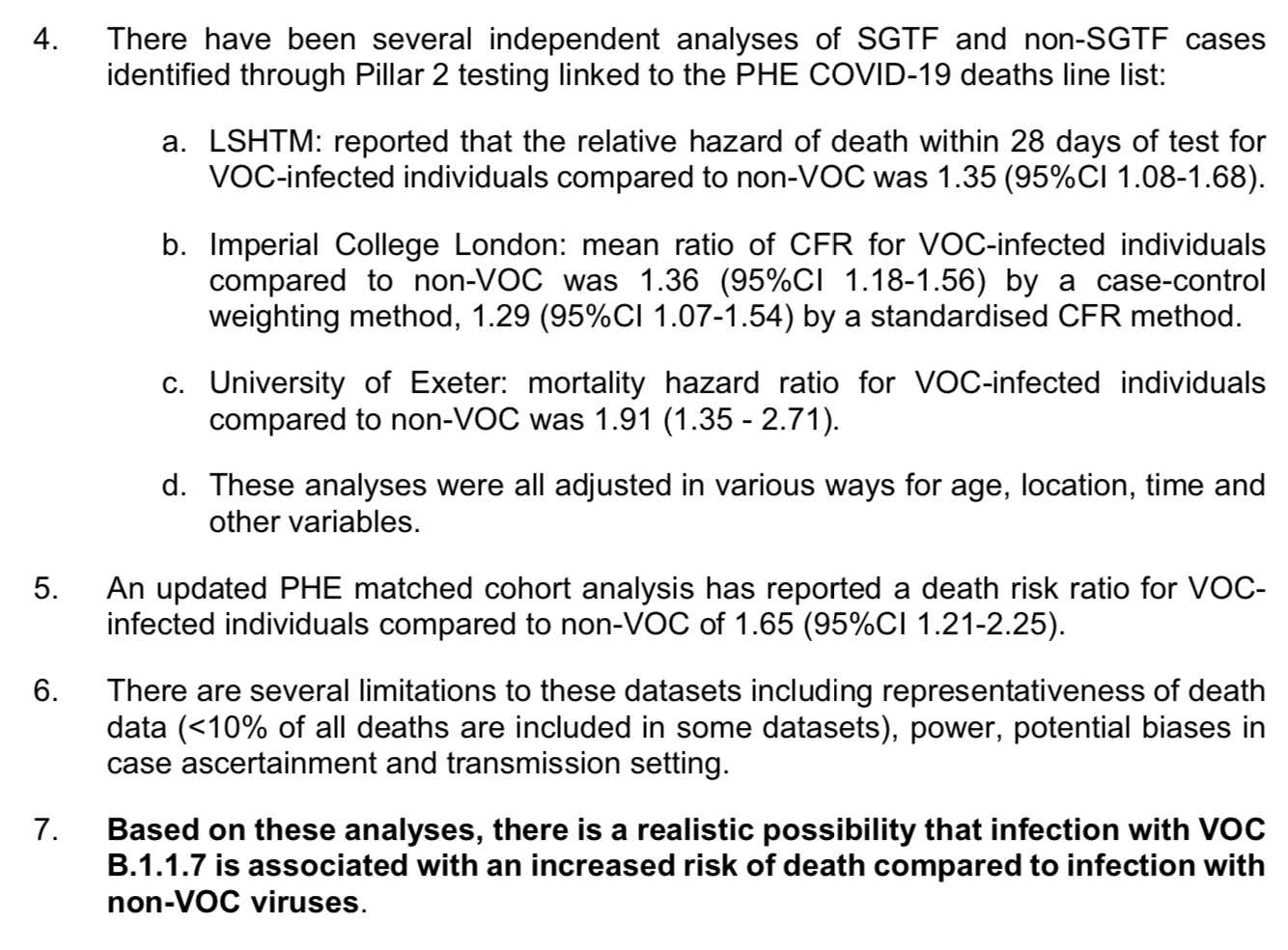
By default, we should expect viruses to become less deadly over time rather than more severe, but more severe is always a risk. We also believe the new strain carries generally higher viral loads, which could plausibly be a cause of higher severity.
I concur with the paper’s level of concern: A ‘realistic possibility’ of increased risk of death seems right. There are a lot of potential confounders here, including time, and the sample sizes aren’t wonderful, so it is too early to jump to conclusions. This is not enough to overcome my prior that increased virulence is unlikely, but given that there is a plausible mechanism to explain it, I’d now put it at something like 40% that there’s substantial (>20%) additional virulence, which I’ve lately been revising upwards.
That would mean that the next few months are all that much more dangerous for those who are not vaccinated. Note that if we do reasonable prioritization the CFR should still drop from vaccinations more than it should rise from the new strain (perhaps not if the Exeter estimate is right, but certainly if the others are right). Remember that nursing homes have tiny populations and cause more than a third of all Covid-19 deaths. But the additional risk to you is real, and compounds on top of the effect that all infections and deaths are divided only among the still unvaccinated and otherwise non-immune.
Construct this with Fauci’s framing of the situation, which suggests all the same actions I’d suggest, but in a way designed to maximize uptake rather than accuracy:

There was also some strange data this week about the new strain in England, hence a lot of this graph was seen:
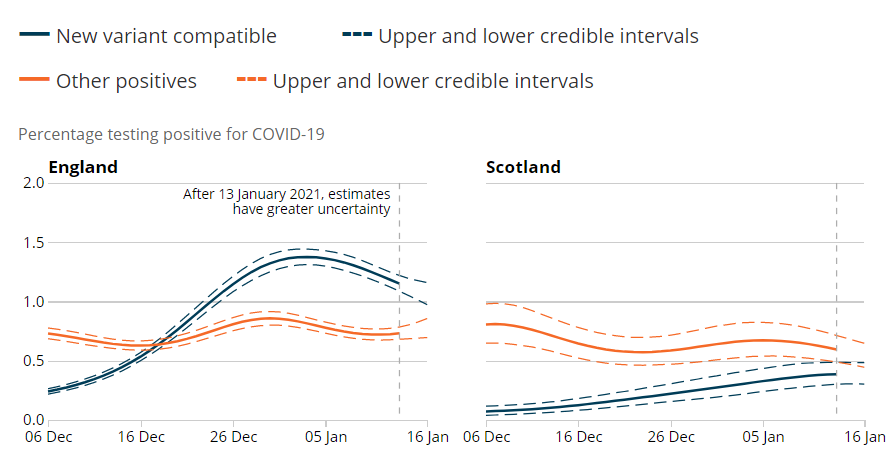
The English graph here seems to show the new strain falling while the old strain is stable, which at first glance is counter to it being more infectious than the old strain. Unfortunately, as one would expect given other data, this seems to be the result of how the data is gathered, rather than reflective of the situation on the ground. If you want to dive in, I’d encourage reading the whole thread:



England is clearly past its peak of infections, but it remains under lockdown indefinitely. Until there’s more people who are immune, there doesn’t seem to be a way to lift the restrictions. So yes, it turns out we can beat the new variant with lockdowns, but it takes longer and is far more painful.
The Other New Strains
It is also accepted now that the South African variant is super scary.
Biden imposed travel restrictions on South Africa this week, which was long overdue. Belgium closed its borders entirely to non-essential travel.
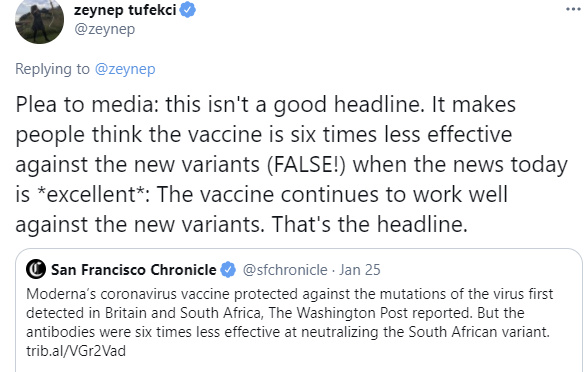
Moderna says it’s working on Covid booster shot for variant in South Africa, says current vaccine provides some protection. This isn’t the best news we could have hoped for, but overall it is reassuring. The vaccines still should mostly work as far as we can tell. The headlines, as usual, often took the maximally alarmist approach.
In case the vaccine stops working, we can tweak it and make a new one. The real questions are still whether we will pay for sufficient manufacturing capacity (yes, this is still an issue) and whether the FDA will throw up barriers for the new versions that slow things down by months.
This headline today tells the opposite story, in any case, excellent all around if accurate:

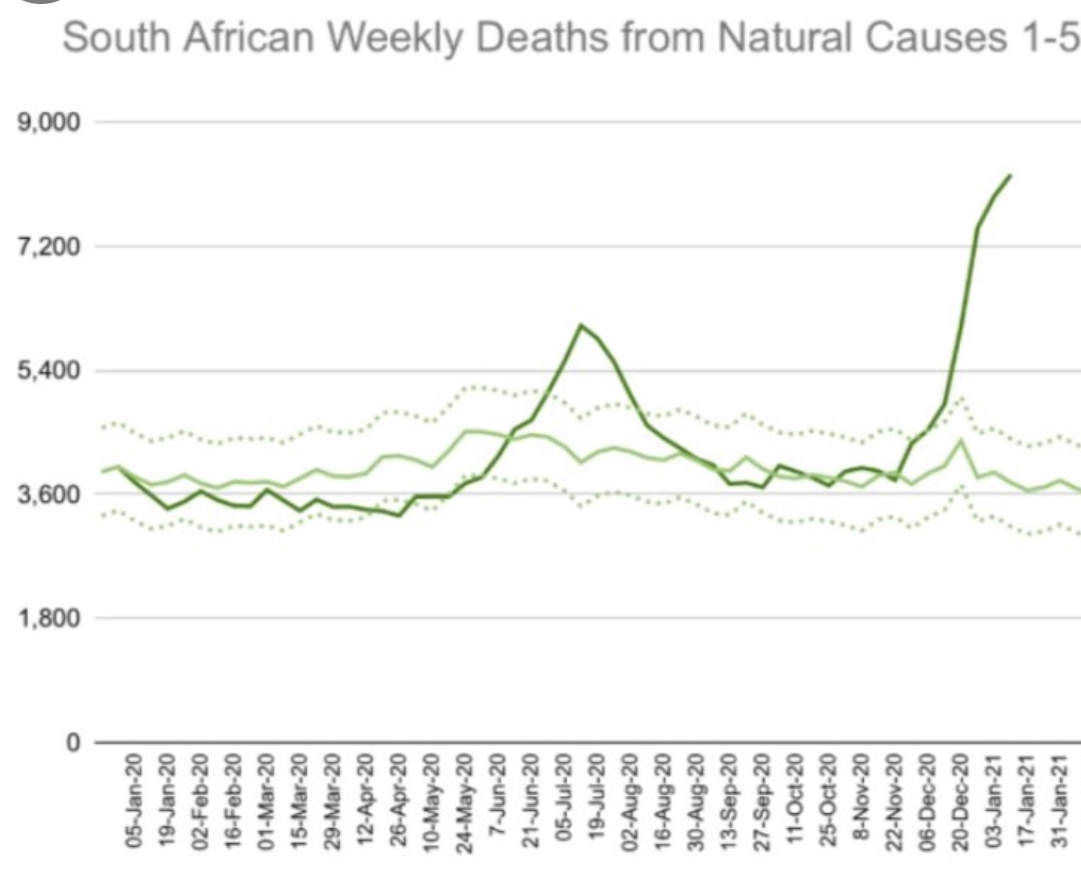
Of course there’s still this graph, of deaths from natural causes for people under 60 years old in South Africa, so yeah we should still go ahead and close some more borders and insist on real quarantines and not make exceptions for citizens as citizenship has nothing to do with how viruses spread, as a prudent precaution:
The South African strain got to Australia, where one quarantining traveller caught it from another while they were quarantining. Hopefully the problem can be contained by having everyone at the hotel in question and everyone who was previously there quarantine again, but it’s a super scary moment.
Developments in Brazil with their new strain continue to seem not great either, especially given how much of the population should already be immune, which continues to suggest easier reinfection by the Brazillian strain.
And guess what? We’ve found our first case of the Brazillian strain in America, in a traveller who was in Brazil. History repeats itself.
This Wired story focuses on who is to blame for the new strains, and says it was our botched pandemic response, and in particular our failure to properly handle the virus in immunocompromised patients. I’ve seen similar other claims elsewhere, but also a lot of objections to such claims, and don’t have a strong position other than that ‘who to blame’ is generally not the most helpful framing.
You know what else scares me? This scares me, because it indicates that Moderna expects to need booster shots, and also sees no path to getting booster shots other than going through all the trial phases over again for each new booster. So they intend to start ‘general booster studies’ in March, and then ‘begin with their phase 3 trial participants’ between June and August, and then have to wait for the data to come in while cases are presumably much lower, and then only after that be able to start production. So the next time we get hit, it may well be many months before we can meaningfully prepare or respond.
What is the New Administration Doing About Covid-19?
It’s now been a week rather than a day. Let’s see how it’s going.
By the standard of the old administration, which seemed to be doing actual nothing for the last several months of its tenure, this was a triumph on day one, I’m making a note here, huge success.
The standard of a benevolent and competent government is somewhat harsher. How’d we do?
Here’s a list of his first few days’ executive orders.
My main take on all these executive orders is that it seems the government is no longer capable of carrying out its basic functions without explicit executive orders, and that seems like a problem? Even when the executive changes it up and does provide the necessary orders?
I’ll skip over the stuff that isn’t pandemic-focused.
Biden signed an executive order to create a National Center for Epidemic Forecasting and Outbreak Analysis. That is the kind of order that makes one wonder both ‘doesn’t Congress control the power of the purse anymore?’ and also ‘What do you mean we didn’t have this before?’ and also of course ‘I take it we won’t be using any prediction markets despite that being the obviously correct way to do this?’ but this still has to be a net win in the long run.
He directed FEMA to expand reimbursement to states to fully cover the cost for National Guard personnel and emergency supplies. It’s scary to think that failure to do this was slowing down emergency supply provision including the vaccine, but this seems to be true. Also, this is a transfer to the states, which is urgently needed.
He signed an order to establish the Pandemic Testing Board to expand US Covid-19 testing capacity. So, points for telling people to expand testing capacity. That’s much better than the previous policy of actively suppressing testing capacity, and likely is a good step to improving our PCR test supply. The problem is that the main obstacle to testing is the FDA banning people from running tests, and I don’t see any signs that this is likely to change much, let alone that preventing this will get the attention it deserves. I’d love to be proven wrong.
He signed an order to establish a preclinical program to boost development of therapeutics in response to pandemic threats. Again, that’s presumably a clear win over not doing that, but again the main barrier to development of therapeutics is that we’ve banned the most efficient methods of developing and testing therapeutics, together with our failure to allow the use of therapeutics. Might want to get on that.
He signed an order to enhance the nation’s collection, production, sharing and analysis of Covid-19 data. Did you know you can just do that? Order such things enhanced, and presto, they’re enhanced? That’s pretty neat. Good idea.
He directed FEMA to create federally-supported community vaccination centers. Good show.
He stopped the USA from withdrawing from the World Health Organization. While the WHO is a proud founding member of the Delenda Est Club, us being outside it likely wouldn’t have made things better.
He directed the Department of Education and HHS to provide guidance for safely reopening schools and childcare and higher education, and directed OSHA to release clear guidance, decide whether to issue emergency temporary standards, and ordered them to enforce worker health and safety requirements, and wait, they all needed to be directed to do that? Isn’t that their jobs?
He issued a directive that CNN summarized as: “A presidential directive to restore America’s leadership, support the international pandemic response effort, promote resilience for future threats and advance global health security and the Global Health Security Agenda.” It seems directives have magical powers? More of us should try them.
He asked Americans to wear masks for 100 days. They should totally do that, but not sure why this is an executive order.
He created the position of Covid-19 response coordinator, which really doesn’t seem like it should require a signing ceremony and a big to-do, and also shouldn’t be required at all in the sense that this implies the position did not previously exist.
He extended the ban on evictions, as expected.
So, if nothing else, major points for nothing being actively unhelpful. You love to see it.
What was missing were the things that were most maximally helpful.
If I was in charge of the administration response, my top priorities would be the first three or four here, then the rest:
- Approval of Astra-Zeneca and Johnson & Johnson Vaccines
- Approval of all reasonable Covid-19 tests, and ramp up capacity.
- Ramping up manufacturing capacity for vaccines, and/or buy more doses, by paying more money
- Enable use of half doses where appropriate, and test even smaller ones.
- Ramping up our capacity to put shots into arms, partly by paying more money.
- Prioritization of vaccinations by age bands only to extent possible, and if possible deprioritize vaccination of those who already had Covid-19.
- Expand vaccine efficiency through half-doses and making sure we use everything in every vial.
- Impose travel restrictions to contain strains from Brazil and South Africa.
From Biden’s first batch, I’d say the job got half-done on #8 (EDIT: looks like he banned people travelling from SA to USA, but not USA to SA and then back again, which somehow doesn’t count, and that’s pretty terrible), and some reasonable efforts were being made on #5, but I didn’t see any of the impactful actions being taken on the other five, especially the first three, which are the ones that matter most.
But then a miracle occurred, and it turned out that yes if you are the United States you can just buy more vaccine doses and then you get more vaccine doses, so we did that!
There are two immediate reactions that come to mind.
The first is, of course, woo-hoo! Best possible news, other than good results from Johnson & Johnson. Everyone’s timelines for normality can move up several months.
The second is, wait, we could have just done this the whole time? Things that, while positive and important, and thank you for finally stepping up, could have been brought to my attention yesterday! The costs of not stepping up on this until now have been staggeringly high.
There’s a lot to do and a lot of fires to put out. A lot of the executive orders that were issued highlight exactly how deep a hole things started in, making it hard enough to merely stop digging. It’s still worth noting that many of the high leverage potential actions are not being taken.
That may be why he said “There’s nothing we can do to change the trajectory of this pandemic for the next several months” in the context of pushing for economic relief. Which is a deeply troubling thing for him to say. Of course there are lots of things we can do! A bunch of the things that Biden did on day one are going to do it. The extra vaccine purchases will definitely do that! We could end the pandemic in the next several months if we wanted that badly enough.
This was HHS’ Becerra attempting to clean up the mess that line created:
I worry that people who think we ‘can’t change the trajectory’ will stop caring about the impact of their decisions on others, since this statement is explicitly saying those actions don’t much matter.
We have serious action on one of our key priorities, expanding supply of existing vaccines. Now we need to push harder on allowing tests and additional vaccines from AstraZeneca and Johnson & Johnson, and on half doses. It looks good for Johnson & Johnson, but we need more pressure on AstraZeneca and on testing, and to put us over the top on half doses.
The Quest to Sell Out of Covid Vaccine
I would feel bad about my massive confusion and inability to figure out how many doses we have, except that I am not alone and this is real.

It’s a giant mess out there. Millions of doses are missing.
Or in layman’s terms:

Logistics is hard, especially when you have no idea what is going on or how much inventory you have let alone where it is or where it is going. And as Yogi Berra said, if you don’t know where you are going, you might not get there.
It is one thing for the White House to not have a plan. We all knew the previous administration did not have much of a plan. It is another thing to completely lose track of what is going on and where you have how much vaccine. That’s kind of impressive.
It is a real question how much this lack of knowledge matters. On the one hand, yes it makes planning on the part of states, counties, sites and people much harder. No one knows how much vaccine they will be getting. On the other hand, aside from having to cancel and schedule pending appointments, it’s not that clear how much value of information is here. What behaviors, other than short-term appointments, need to change? Should capacity be different based on existing supply, or (as I’d strongly suspect) does it almost entirely depend on the pace of future supply?
One danger is that doses might be held back en masse more often as second doses when they could be used now as first doses, because there is no confidence in future deliveries, delaying the whole process and increasing risk of spoilage. In some places this is clearly happening.
Still, the good news is that the core behaviors don’t change. Use what vaccine you have to vaccinate people, get shots into arms, expand capacity and be ready for when there is more vaccine later. Uncertainty certainly can interfere with the incentives and motivation to expand capacity, but my understanding in at least most places is that this won’t impact the important practical barriers to expanding capacity, since they’re almost entirely regulatory limitations and other rules from on-high combined with time required to set things up, and getting vaccine to distribute even once is enough to set up the capacity involved, so long as it doesn’t sit around unused for way too long afterwards.
The uncertainty involved here is not great, but given that we also have high uncertainty about our manufacturing capacity and how many new doses will be available in the future, it’s not at all clear to me that this is a substantial additional burden or that it will much impact our long term path. Mostly it’s deeply embarrassing, in a #YouHadOneJob sense.
So while noting that ‘as far as we can tell’ is not all that far, as far as we can tell, how is it going?
Compared to before, I’d say pretty well:

The details, though, are contradictory and hard to sort out.
Bloomberg says that only a few states have managed to use over 80% of their vaccine allocations, and none have used over 90%. They have New York as having used 58% as of January 24.
Cuomo vehemently disagrees, and says the state is fresh out, and certainly the state has been cancelling appointments like they’re fresh out:
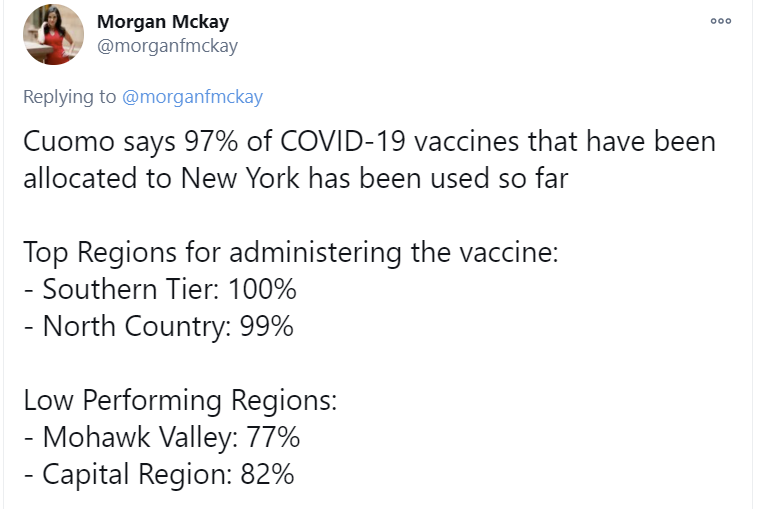
(This looks weird, so I checked: The Capital Region is 1.17 million people, Mohawk Valley is 432k people, and NY overall is 19.45 million people, so those two regions would have the majority of unused doses if Cuomo’s numbers are correct here.)
The difference between 58% usage and 97% percent usage is rather large.
If it is a reporting lag issue, it is a rather large reporting lag issue, and would presumably be and imply excellent news about distribution.
If the rest of the doses are truly gone, then New York has managed to throw out a full third of the doses we were given, and that should likely be the biggest scandal of the entire pandemic. Heads would need to roll, ideally literally. We’re terrible, but I do not think we are that terrible.
The other possibility (that doesn’t involve anyone lying or committing fraud) is that this is an interpretation issue. In that scenario, New York State is reserving second doses and calling those vaccines ‘used’ whereas the official tally notes they haven’t been used because they haven’t been used. If that’s the case, then about 39% of doses are reserved this way.
Using Bloomberg’s numbers, New York has given about 88% of its delivered shots as first doses, or 1.4mm out of 2.4mm allocated doses, so the math would work if the difference is the reservation of most second doses. It does seem that this is largely the case, with Cuomo saying the use of second doses (that are in storage) as first doses is ‘up to the federal government’ which I’m guessing is true in practice if and only if Cuomo decides that it is up to them. I also know that not all second doses are held in reserve, because I know someone who has a second dose appointment but no confirmed second dose, and the site reports having cancelled some second doses for lack of supply.
Virginia is an example of a place that is both not selling out and also not supplying vulnerable people with the ability to get vaccinated:
I talk about New York a lot because New York has a lot of reporters, Cuomo gets a lot of extra attention, and also I live in New York. Virginia is highlighted here because that’s where George Mason University is, hence the attention from Marginal Revolution. No doubt there are lots of other disasters in other places that are getting less attention.
Kittarus County in Washington claims to be doing extraordinarily well, with zero doses wasted and 95%+ distribution within a week of getting doses. They did it exactly the way you’d expect, by having experience with other disasters, and doing the work of finding people to vaccinate, while going down the priority list as needed when they had extra shots. One thing not mentioned is how efficient they’ve been extracting extra doses, since ‘no doses wasted’ could imply insufficient attention to that factor.
West Virginia and Alaska still win the crown. They might not have quite given 110%, but WV is still claiming to be at 101.4% at least for first doses, and are well ahead on percent of population vaccinated:
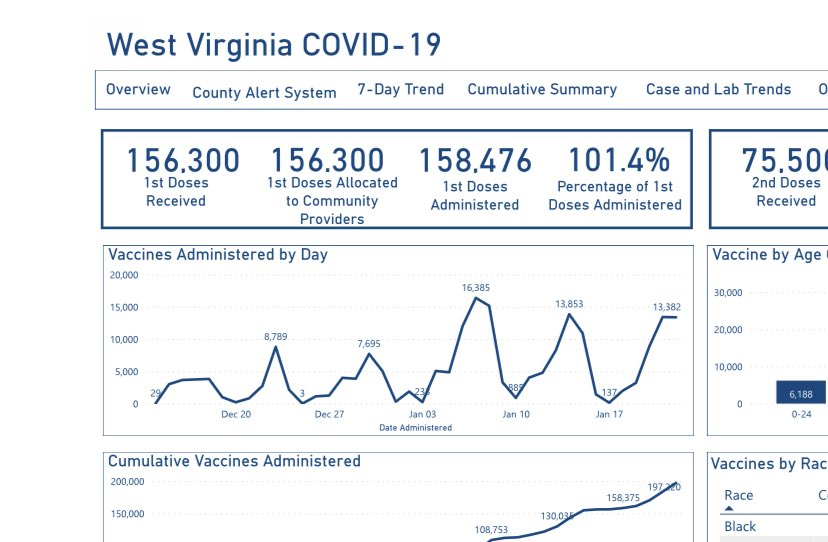
The way that graphic is organized makes it clear that there are generally two sets of books being kept, one a percentage of doses administered and the other a percentage of first doses administered, and a lot of the confusion is that the two measures are being frequently conflated.
The Quest for More Vaccine and More Vaccines
Johnson & Johnson’s vaccine is potentially a true game changer. It is one dose, does not require special temperatures, and they are claiming 100 million doses by the end of April. Fauci is now on record expecting a decision on the vaccine by February 7 and general expectation is next week. What’s confusing is that it seems that the process is now something like, first we get the data, then we analyze the data, then we make a decision – so far so good – and then we apply for Emergency Use Authorization.
This seems accurate to me. First, data is gathered, then the data is analyzed, and once everyone agrees that we should grant approval, then we apply and a meeting gets scheduled for several weeks later. I hope to be wrong and pleasantly surprised.
Then again, this isn’t the biggest deal, if J&J is truly ‘going all out’ in its production capacity. They’re looking to have 100 million shots (of their one shot vaccine) available by April. Snags will mean it is going to miss its goal of 12 million doses available in February. It would be much better to get those shots into arms in February rather than March, but the key is to create as many shots as possible and then put them into arms. I am confident that we’ll be able to catch up, and get all the shots into arms quickly once approval does come, now that supply is rapidly becoming the limiting factor.
Meanwhile, Pfizer has decided that since we’ve managed to extract more doses out of their vials, that means they’ve delivered extra doses, and so based on their contract they can ship us less vials, as they did with Denmark:
I have zero problem with Pfizer getting paid for the extra doses. I’m actively in favor of that, as I do not have a fear that someone, somewhere is making a profit. What I definitely have an issue with is them delivering less vials to us as a result, especially if they then use this as a reason not to ramp up production, or ship those doses instead to places that aren’t extracting the extra doses and instead throwing them out. This seems like a very easy compromise to have struck – we agree to pay for the extra doses, Pfizer agrees to still give us all 40 million vials.
Scott Gottlieb makes an interesting defense of Pfizer’s move here, that only by giving everyone no choice but to use the extra doses, can they ensure that the extra doses get used:
There was then a big to-do about the fact that the syringes necessary to extract the extra doses often aren’t being provided, and thus the extra doses couldn’t be extracted and thus shouldn’t count. This of course points out that the extra doses were being wasted by this before, and Pfizer only fixed it when it got them paid. Which is exactly why you want to pay them for the extra doses. If it got the syringe problem fixed it was worth ten times the extra cost for that alone.
I fail to see why shipping less doses is necessary to get maximum uptake, given there’s a massive shortage either way, and it doesn’t seem like this will prevent all the vials from being distributed, which is the only thing that matters. I hope.
The key as always is to keep the vaccine flowing as fast as it can be manufactured, and to ramp up that speed of manufacturing as fast as possible. Payment is one thing, but decreasing vial allocation to people who efficiently use the vials they get is a rather low and destructive thing to do, and it would be unwise to tolerate it.
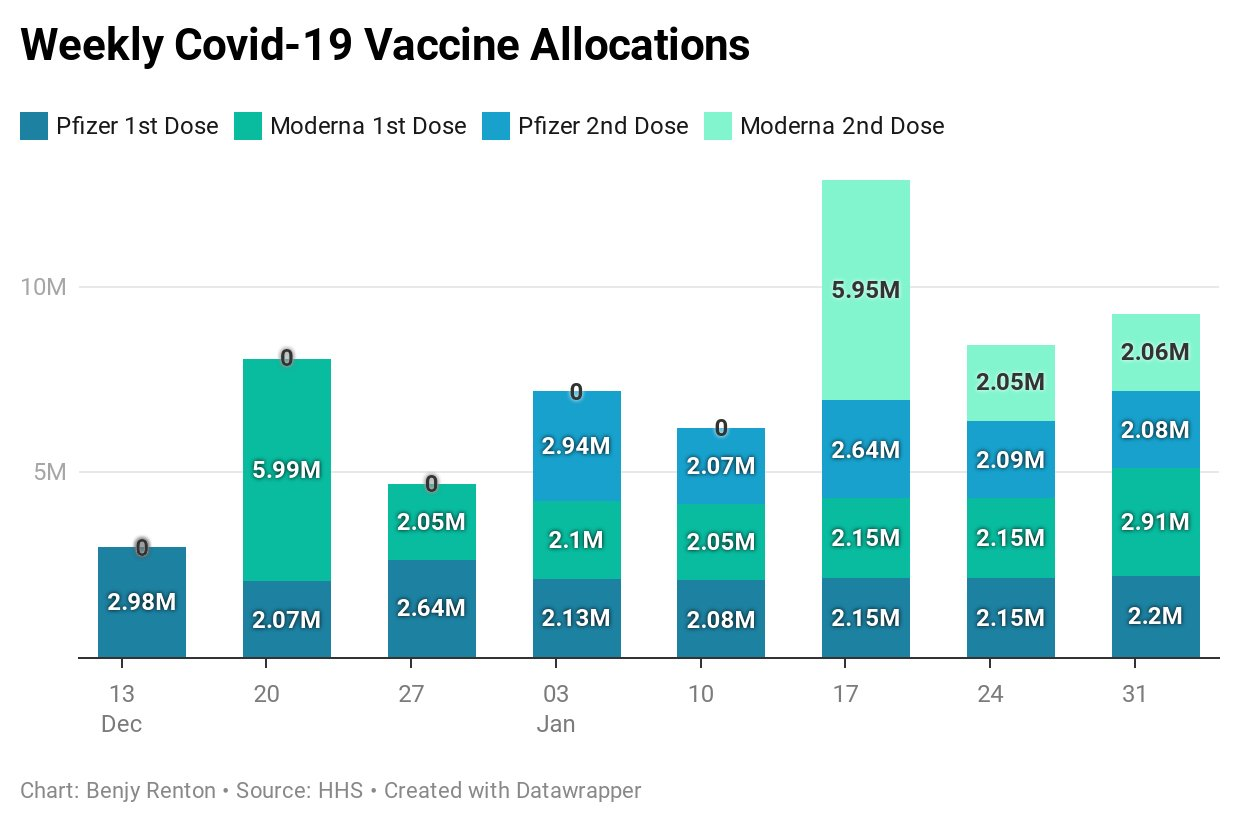
In the short term, looks like supply will be increasing slowly, but definitely increasing (WaPo):
Pfizer also going to deliver doses faster than expected (Bloomberg).
In ‘actually being helpful’ news, while they wait for their own candidate to become ready, Sanofi to produce 100 million Pfizer vaccine doses, CEO says. The ability to profit from the deal allows Sanofi to take helpful action here, which is excellent. Could we get anyone else to follow suit? How about Merck, whose vaccine unfortunately didn’t work out and was cancelled this week due to lack of immune response?
AstraZeneca meanwhile is suffering supply problems, and cut their first quarter allocation of vaccine to Europe by 60% this week. I hope that they’re giving Europe all the doses we’ve refused to approve here in America, so they’re not sitting on the shelf unused. It’s kind of weird that we took one of the most promising vaccine candidates, and made an exclusive deal with one pharma company but required them not to make a profit until after ‘the pandemic is over.’ Might not have been the best incentive structure Oxford had available. I thought the chaps there were smarter than that.
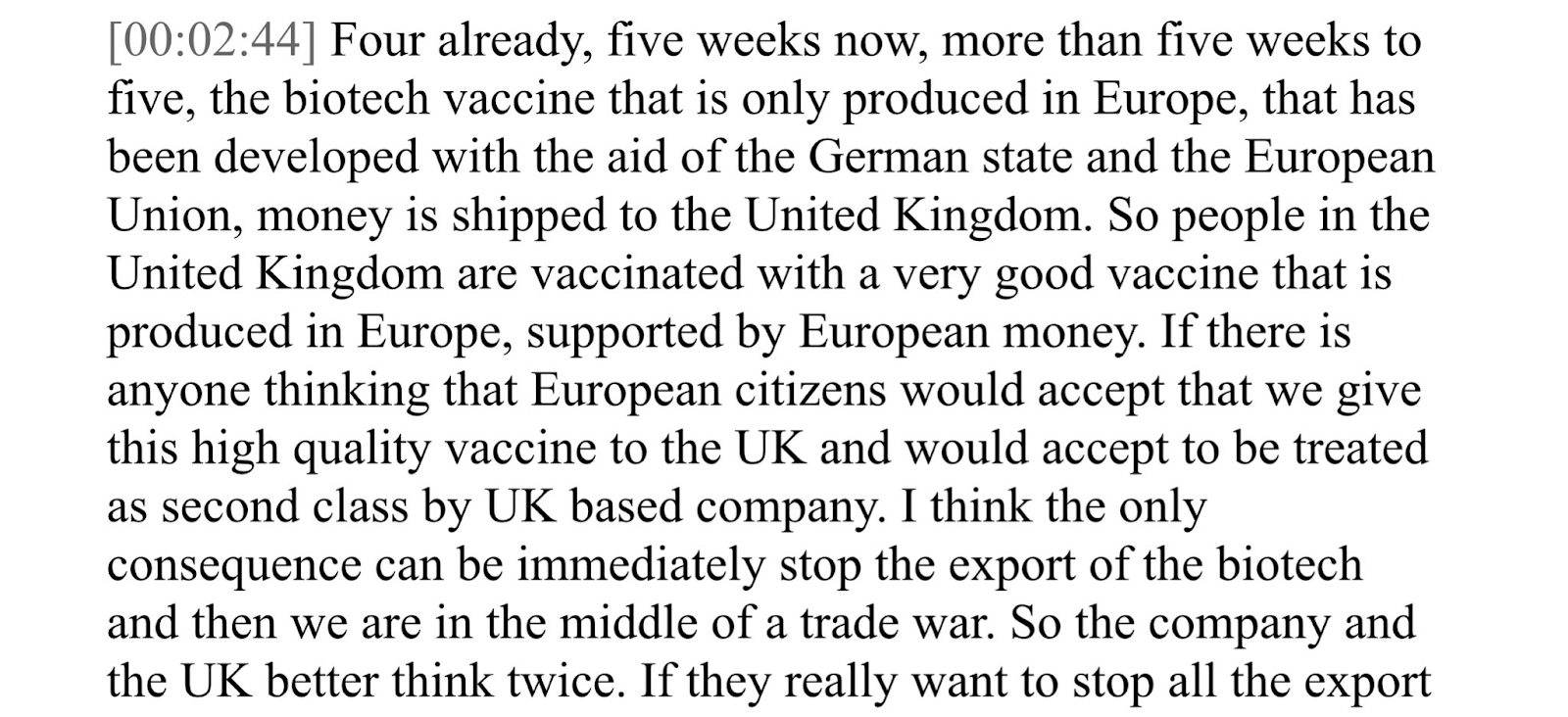
This led to a fight between the EU, UK and AstraZeneca, because the EU wants you to know that when they pay for second class vaccine distribution three months late, they will not be treated as ‘second class citizens’ and the UK ‘better think twice’ or they’ll prevent the vaccine from being shipped:
Meanwhile, they haven’t even approved the vaccine in question yet.
And they are saying that when they do eventually approve the vaccine they’re rattling sabers about not getting, they might not approve the vaccine to older people, because they have a “limited amount of data” on that subpopulation.
Germany has gone ahead and done exactly that, recommending the vaccine only to ages 18-64 and not to the elderly, those years becoming ever more the magical talisman.
Don’t get me wrong, AstraZeneca absolutely messed up their trials in several ways and this is one of them, they’ve been a disaster as good vaccine candidate shepards, but punishing the world to spite AstraZeneca’s face in a way that mysteriously lets them make more money because they get paid higher prices for later sales doesn’t seem like a punishment that fits the crime.
I’m also worried that it is possible that no one in the trial was named Erica, so perhaps it doesn’t work on people named Erica. Please, Erica, consider whether this is safe. Erica?
One Dose, Two Dose, Half Dose, Who Knows
The ultimate low hanging fruit in expanding vaccine doses is to give half doses of vaccine to young healthy people, thus greatly expanding supply. We know that the Pfizer and Moderna vaccines generate robust immune responses in young people when given two half-doses, similar to that for full doses. That second half of each dose is what was used in the Phase 3 trials, so it is what we are doing, but it is mostly wasted. I would happily accept two half doses earlier, rather than two full doses later. And that’s exactly the choice we have to make.
Vivek Murthy, who is playing a key part in the Biden Administration’s response, said on a podcast with Ezra Klein that his concern is with the duration of the vaccine response from a half dose, because “we don’t know” (which is another “there is no evidence for”) that the response will be as long lasting. Maybe it fades away faster, you see, and then we’d need to use more vaccine in the future. Which is nonsense. If you generate the same response there’s no reason to worry that you’ll then remember it was from a half-dose and fade away in a few weeks. Like all such FUD concerns, I suppose it’s theoretically possible, but come on. He also suggested a similar set of FUD about delaying second vaccine doses, saying “science from other vaccines shows us there is a risk it won’t work and will require revaccination.” Whereas everyone who actually looked at other vaccines, that I know of, thinks that risk is minimal.
Vivek also used the term “driven science” as code for “anything not in a proper study isn’t evidence.” Ezra correctly pushed back hard on this, asking if “following science” meant only “certainty.” Vivek thanked him for the question, said no we look at all the available information and make the best decision we can, and entirely disregarded the contradiction.
On the other hand, he was quite promising on questions of rapid testing:
We have great news. Half doses are being seriously considered for at least for Moderna! Talks have begun with the company. I don’t see why this needs to be up to the company. All we have to do is allow professionals to give out half doses to people under the age of 55. I suppose Moderna wants to be paid for the half doses as if they are full doses, since they are “doses” and they’re paid by the dose, and of course I do not care about that at all, pay the money if they ask for it. Because that matters almost not at all.
The real question is, why stop at half doses? If a half dose and a full dose work equally well, the next logical question is, what does a quarter dose do?
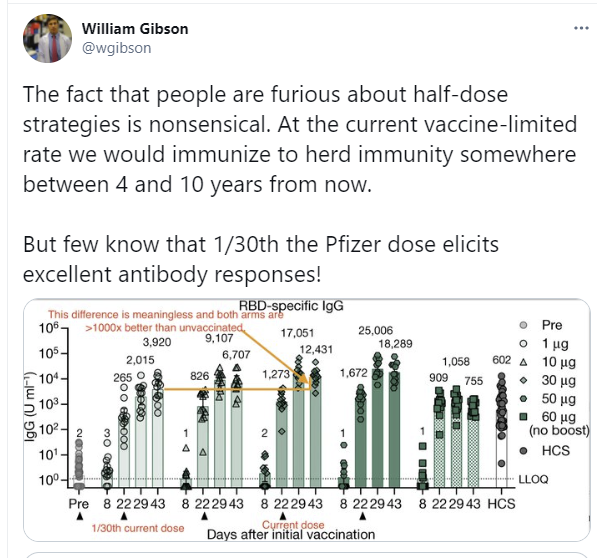
Upon further analysis, I think he’s going too far. I do not agree that the difference here is meaningless, or that there are no downsides to giving only one microgram instead of thirty or fifteen.
The first thing to understand is that this is a log scale of immune response. Lines that don’t look that different can represent substantially different levels of response, and the tiny dose is definitely not going to always get it done.
Another issue is that when you give the immune system a very small stimulus, this can be interpreted as something to ignore, and tolerance can result. Thus, if you give very small doses, it risks messing up your immune response. This would be very bad, and is a real risk if you push too far.
None of that means that we shouldn’t test tiny doses. We should certainly test quarter doses, and do more testing on half doses if we think half doses require more testing, and once we verify quarter doses are good check eighth doses to see what happens.
What this all definitely drives home, once again, is that we have had it in our power the whole time to put a stop to all this.
Vaccine Allocation by Politics and Power
It matters who you know. Someone I know managed to become known to someone in a position to have information on vaccine supply, and placed a call. The person in the know is going to alert my associate to new vaccine shipments in their local area, so they can call around and make an appointment before others can do so. That’s how such things go.
If you are going to complicate the process of vaccination in order to do better prioritization, the most obvious group to exclude are those who are already immune. Vaccine given to an immune person is vaccine wasted, and that’s one person in four. Giving people antibody tests before vaccination thus makes a lot of sense.
The problem is that even this maximally useful policy would dramatically slow down vaccinations, as it places another barrier into the process. In theory it’s great, in practice this would backfire. A lighter version of the suggestion is to exclude those with known prior symptomatic Covid-19. I’d urge those who know they have already had Covid-19 to wait on their vaccinations until we have enough supply for whoever wants it, but I wouldn’t introduce any formal rules or checks on that basis.
The long term care facilities still aren’t getting their shots into arms. It’s going rather epically badly, and not appreciating the extent until now is one reason why I undershot the death count this week by so much:
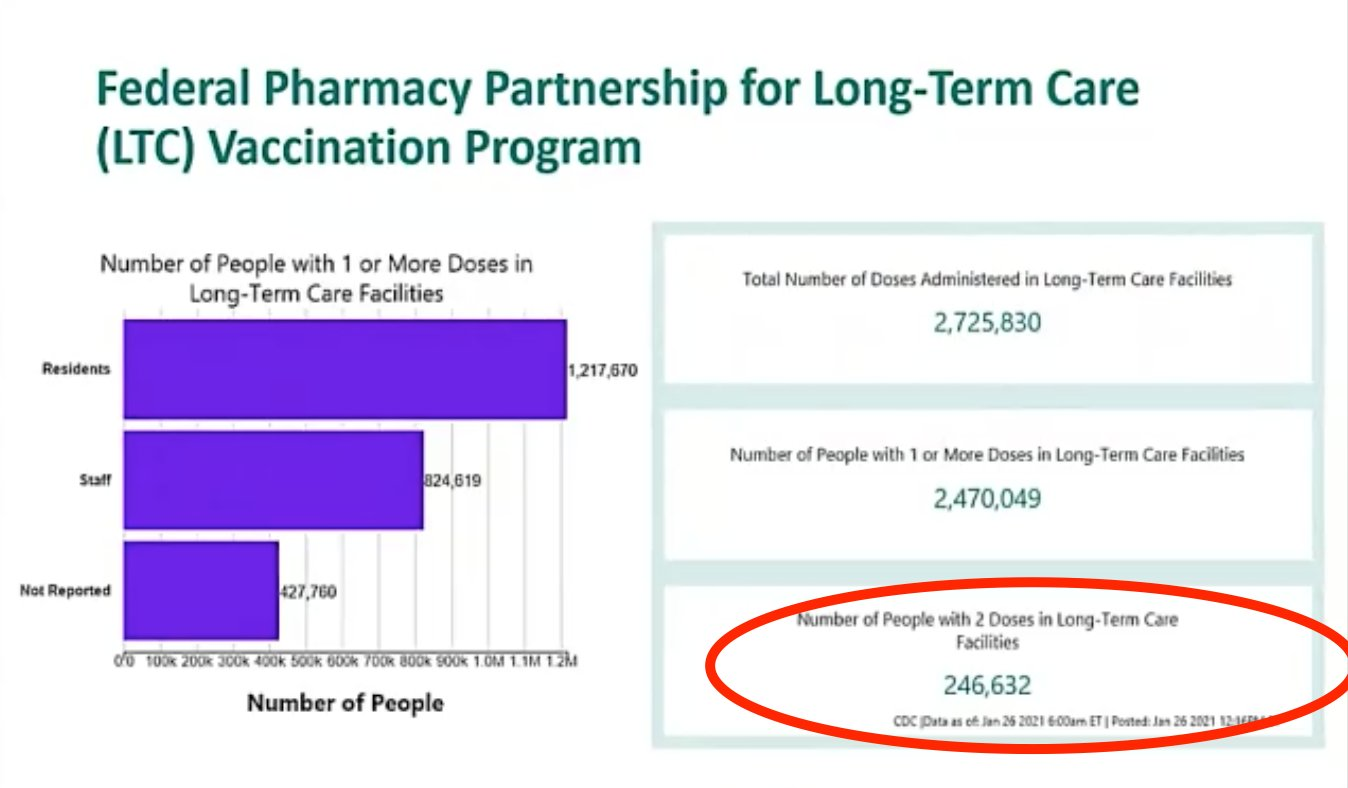
The partnership with CVS and Walgreens does not appear to be working. The question is why. My presumption is that we’re asking CVS and Walgreens to do exactly what they don’t normally do, and go other places to deliver medicine, rather than asking them to give shots in their stores which is what they know how to do.
At the time, I was happy to see any use of such resources to administer vaccines. That was a mistake, and I should have been more suspicious that they were given exactly the contract they were not suited to handling, because they were not suited to handling it, thus choosing ineffective action while allowing blame for failure of the one key action item to be reallocated and claiming partnerships with companies with reputations for effectiveness. While providing no real incentives for these companies to deliver the goods. Quite the trick.
Stop Living in Fear After Vaccination

The vaccine protects against Covid-19, better than we could have hoped for. Every data point we get reinforces that. Over a hundred thousand people, mostly elderly, and zero serious cases.
As per previous findings, big drop starts on day 14 after the first dose, which includes the standard testing lag and is a seven day average, but yes you need the second dose to get full effectiveness.
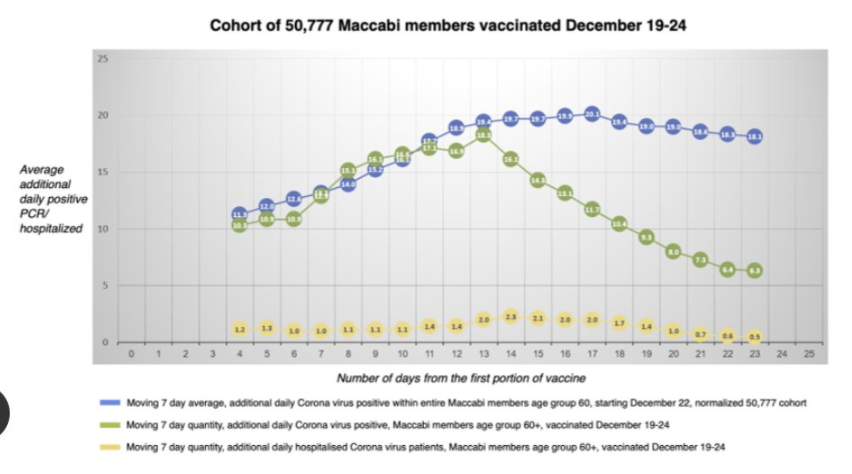
Remember that PCR tests often come back positive for a while after you are sick, so it’s likely many of the 20 positives happened before the second shot had its effect. And remember that for young people the shot will be far more effective than this.
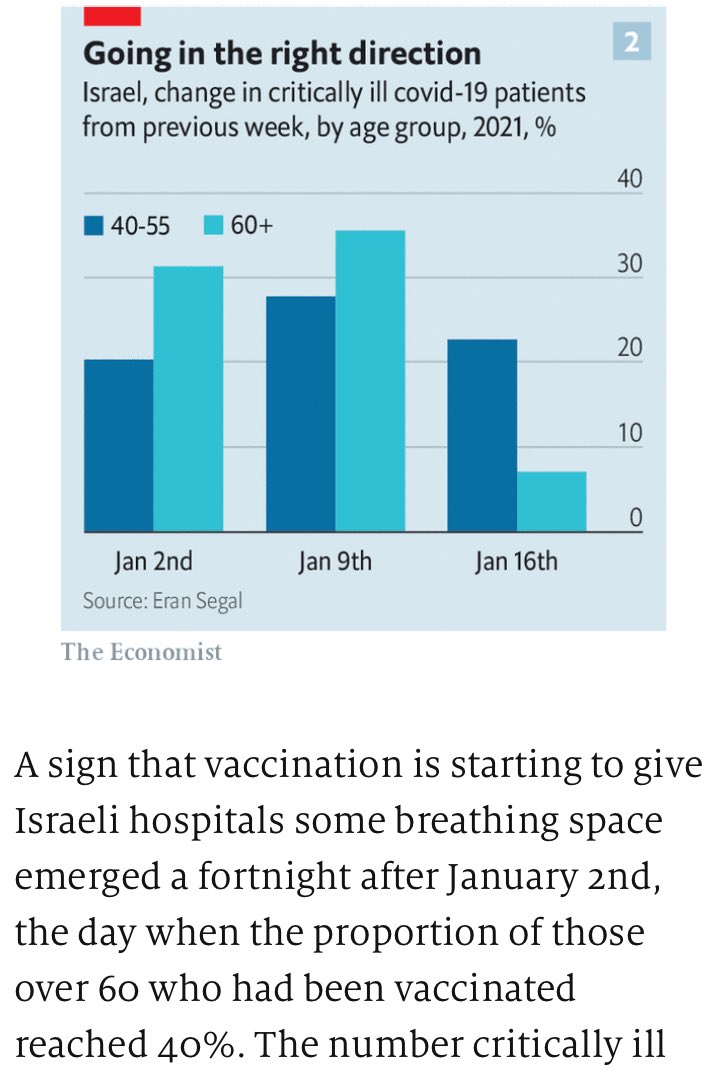
Here’s what happens when you vaccinate old people first, keeping in mind coverage is far from complete:
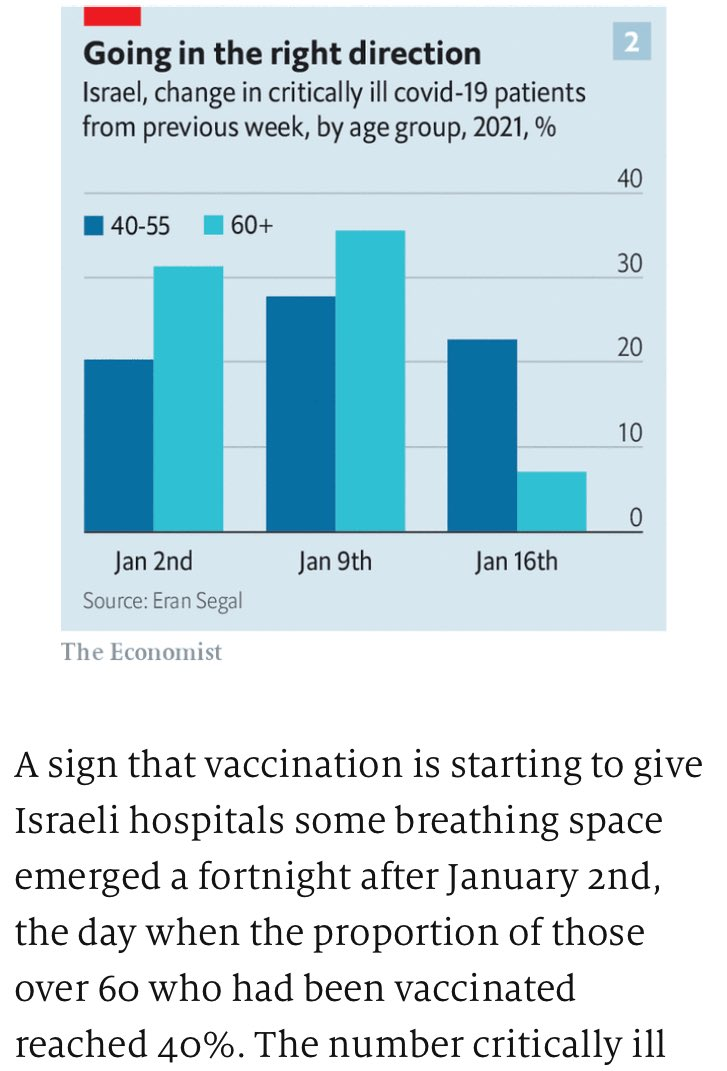
I am not a doctor and nothing anywhere in any of these posts is medical advice, and everything in this section is definitely not medical advice, but seriously. The vaccines work.
If you’re fully vaccinated, please do keep wearing masks, and otherwise reinforce good pandemic norms. But don’t keep putting your life on complete hold, and especially please do not keep freaking the f*** out about Covid-19 risks, especially the risk of you infecting others.
All around me, I see people who have been vaccinated needlessly freaking out, or freaking others out, about Covid-19 exposure.
A vaccinated person I know is freaking out because their personal trainer tested positive, they had a 25-minute session with them mostly more than 6 feet apart, and they are worried they caught the virus then and will spread the virus to others.
A distinct vaccinated person I know saw a friend of theirs, and now has to get a Covid test before someone else will agree to see them a week later.
A distinct vaccinated person I know is planning to travel and see others, and people around them are freaking out about this as an unsafe act.
The talking point that “we have no proof that vaccinated people can’t spread the virus” is successfully freaking out a lot of people who really, really should know better.
Here is PoliMath ranting about the whole situation. In addition to the central point that vaccinated people are in the worst case very, very poor transmitters of Covid-19, the second point, that saying the technically correct statement “X may be possible” in such situations is deeply misleading and irresponsible, cannot be emphasized enough.
None of this makes sense in terms of the magnitudes of the risks involved.
It all makes a lot more sense if what people cared about all along was whether they are blameworthy for creating “risk” rather than caring about the spread of Covid-19. If people have mostly been LARPing a pandemic rather than caring about who gets sick. Now that the actual risk is mostly gone, the act continues, because blame for “risk” is a binary and the actions in question still get instinctively processed as “risk” and people wish to instead remain in a state of grace, either in their own eyes and/or the eyes of others. Morale remains low, so the motions continue.
The motions can (mostly) stop. By all means, keep your mask on around the unvaccinated, do social distancing with respect to the unvaccinated whenever and to the extent it’s reasonable to do and avoid needlessly risky interactions. But demanding tests or continuing to fully distance is pandemic LARPing.
And if both of you are vaccinated, yeah, within reason do whatever you want. This article, entitled “Vaccinated People are Going to Hug Each Other” and likely previously titled “Giving People More Freedom is the Whole Point of Vaccines,” another good title, doesn’t add much new info, but is good on this.
Calling this a moral panic seems exactly right to me.
I don’t know what the ‘intractable health and labor challenges” are of keeping schools open when all adults involved are vaccinated, but that seems to be where we are, somehow:
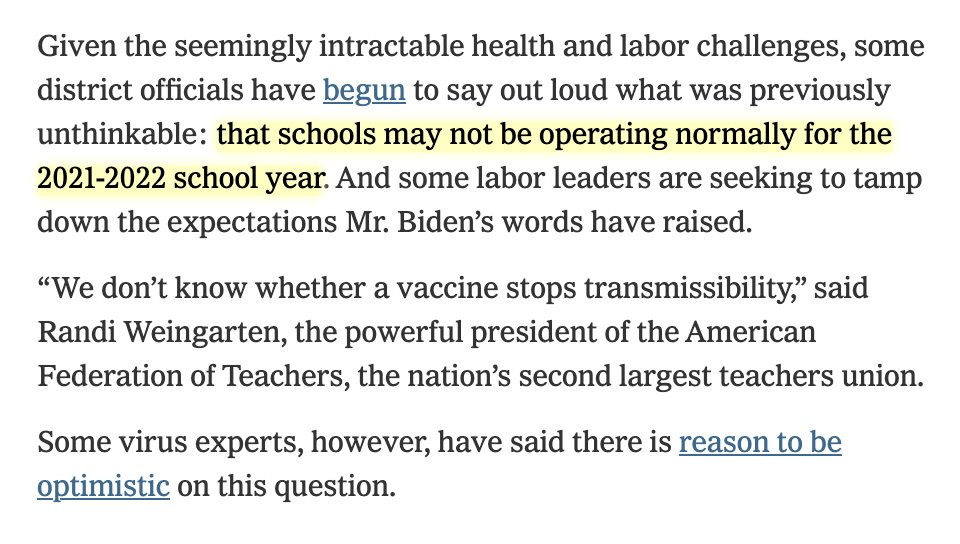
For the most extreme cases of all, I’ve seen reports from several places of support for suspending schools indefinitely even after teachers are vaccinated. Here’s the most stark one of the bunch:

Given what I think about schools, I have mixed feelings about such stands, but if I instead felt as almost everyone does that school is highly valuable to children rather than primarily a prison sentence, I would treat such responses as insane. The FEA here is saying that even if all teachers are vaccinated, and also the pandemic is mostly over, the schools should remain closed until the students are vaccinated, despite the students being at almost zero risk even if they get infected, and the chance of anyone getting infected in that scenario being very close to zero.
If you’re going to close the school for that level of risk, you should go ahead and permanently close the school and also hide in your house with your doors locked.
The teachers (such as these in Maryland) who are objecting to current calls for schools to open now have a much better case. It’s definitely not safe out there and the vaccine is on its way, so the push now to reopen schools that have been closed for a long time seems rather perverse.
Biden is usefully leading by example, attending church services in person now that he is fully vaccinated. Needless to say, he is at very high risk, and it is quite important to keep him safe. The press seemed to focus on his choice of church, rather than on the decision to attend at all, because of the general ban on things that might cause people to take more risks, including after vaccination.
Sports Go Sports
The NFL season is one game away from over. Early on there were constant cries of how crazy it was we were playing football. With each postponed game the cries of ‘how can they think they will play this season’ rang louder. And there were indeed some rather stupid games played on occasion. But here we are, at the end of a mostly normal NFL season, getting ready for a good old fashioned Good vs. Evil Super Bowl.
The same applies to college football. Yes, we lost a lot of games along the way, and several leagues had the self-inflicted wound of starting late, and the virus seemed to sideline my team’s entire offense, but mostly we got to have our season and all the joys that come along with it.
All of that applies despite the Covid-19 situation being vastly worse than the situation at the start of the season, and it was all done without a bubble. Perhaps the virus can indeed (mostly) be contained. How did we do it (CDC link)?

The NFL did it by learning from its experiences and early mistakes, doing the math, figuring out what was actually risky, and using testing, mandatory masks, contact tracing and quarantines. The CDC report is worth reading in full, here are some key passages:
“Midseason, transmission was observed in persons who had cumulative interactions of <15 minutes’ duration, leading to a revised definition of high-risk contacts that required consideration of mask use, setting and room ventilation in addition to proximity and duration of interaction. The NFL also developed an intensive protocol that imposed stricter infection prevention precautions when a case was identified at an NFL club. The intensive protocol effectively prevented the occurrence of high-risk interactions, with no high-risk contacts identified for 71% of traced cases at clubs under the intensive protocol. The incorporation of the nature and location of the interaction, including mask use, indoor versus outdoor setting, and ventilation, in addition to proximity and duration, likely improved identification of exposed persons at higher risk for SARS-CoV-2 infection. Quarantine of these persons, along with testing and intensive protocols, can reduce spread of infection.”
…
“Over the course of the monitoring period (August 9–November 21), 623,000 RT-PCR tests were performed among approximately 11,400 players and staff members; 329 (approximately 2.9%) laboratory-confirmed cases of COVID-19 were identified. After intake screening,¶ in August and early September, fewer than 10 COVID-19 cases were identified per week for the following 7 weeks (Figure), during which time the standard protocol was in effect, which emphasized physical distancing, masking, limited numbers of persons in specific areas, and other important behavioral and facility-related parameters. However, during September 27–October 10, a total of 41 cases were identified among players and staff members, 21 of which were believed to have resulted from within-club transmission at a single club, requiring closure of that club’s facilities. Subsequent contact tracing identified multiple instances of transmission that likely occurred during <15 minutes of cumulative interaction within 1.8 meters (6 feet). Among the 21 persons with suspected within-club transmission, 12 had no device-recorded interactions of ≥15 consecutive minutes with a person with confirmed COVID-19, including eight who had no interactions >5 consecutive minutes and seven who had no interactions >15 cumulative minutes per day (with no other known exposures to a person with COVID-19).”
If you want to dig into exactly how Covid-19 spreads, this seems like a great natural experiment and data set to dig your teeth into. The number of positive tests still went up as conditions in the country got worse, but the problems within the league seem like they were well-contained by the protocols.
The NFL shows what you can do the hard way. The NBA is more ambitious, playing its playoffs in a bubble, and now using trained dogs to detect Covid-19 for fans looking to attend games. Canine sniffing is a known detection technology that should likely be seeing widespread use, so once again the NBA is showing us what in a saner world would already be standard procedure, because they’re not afraid to look a little weird.
You Should Know This Already
Masks are great, premium masks are better. If you haven’t already, it’s time to step up to at least KN95s. I actually find them more comfortable than cloth. Also a reminder to take your Vitamin D.
In-person higher education spreads Covid-19 and no our precautions are not adequate to stop this (study):
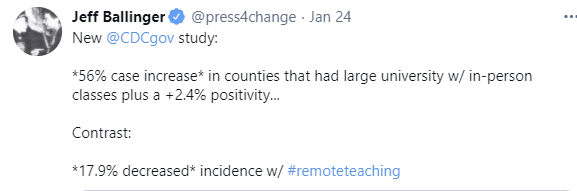
A lot of that is probably population effects, but given the effect size this seems too large for that to explain this away. That doesn’t mean this isn’t worth it. If it’s worth four years of everyone’s life and saddling them with life-crippling debt, who is to say whether a disease students can mostly shake off should be where you draw the line? The students mostly don’t seem to think that. Note that this doesn’t mean that it’s impossible to safely run an in-person college, only that a lot of them did so highly unsafely.
There are libertarians in a pandemic, who periodically point out that the government needlessly blocking private action is entirely responsible for the whole pandemic, and who have many helpful ideas on the margin. They banned tests. They banned experiments and they banned challenge trials. The Moderna vaccine was designed in January. Never forget.
Even most relatively smart people fail to appreciate the benefits of forecasting. They instinctively seek to avoid information, because information causes Not Okayness and blameworthiness. And one usual reaction to anything you want to shut down is to force it to show its concrete benefits, and then only count the benefits that can be proven and quantified. Whereas in my culture, the quest to get good forecasts is useful in so many different ways. Not only do those forecasts have humongous value of information compared to the cost of getting them, but the act of figuring them out causes us to learn all sorts of useful things and train all sorts of useful skills, gives us valuable discipline and a proper tax on bullshit, and allows us to identify valuable sources of future information. Among other things.
It is one thing to not exclude the previously infected, it’s another thing to actively encourage them to try and get vaccinated during an acute shortage, but then again, Andrew Cuomo is the Worst:
Periodically there will be claims of “no evidence” to stop people from doing obviously correct things, such as delaying second doses for 12 weeks in the UK. In this case, there’s actually tons of evidence that such delays are highly unlikely to be an issue, and the objection is pure fear, uncertainty and doubt about all deviations from the exact thing done in a study rather than the result of any serious engagement with the physical world. I really wish we could reverse the “no evidence” thing back at such folks effectively. There’s definitely “no evidence” that a 12-week delayed dose is less effective, and also there’s no Baysian evidence either.
Poorly ventilated spaces spread Covid-19 highly effectively, and make talking highly dangerous. Strangely I didn’t see an obvious link back to the actual study, even on the Royal Society webpage, but the findings are no surprise.
How we usually do Covid-19 ‘safety protocols’ as a nation:
This seems to be the standard pattern. Take the valuable activity and both require it and limit its supply because of social distance, thus forcing people into lines and otherwise into confined indoor spaces that result in a lot more risk rather than less. The supreme version of this was of course the completely NYC-subway-style-packed airports back in February, but ordinary disastrous versions of this are everywhere.
Whereas here’s how China rolls, leaving nothing to chance:

I strongly suspect that the new tests are being favored because of the inconvenience rather than in spite of it, thus implicitly appealing to regime sensibilities and the accompanying unambiguous signal that they mean business, and given that the justifications for their improved accuracy don’t seem great. Still, dedication, man. They have it.
Life must be lived and frequent testing helps a lot, but if you act like this (pictured include Dave Chappelle, Joe Rogan and Elon Musk):

Then there is a good chance that at least one of you is going to soon test positive for Covid-19, which Chappelle did. Balance in all things.
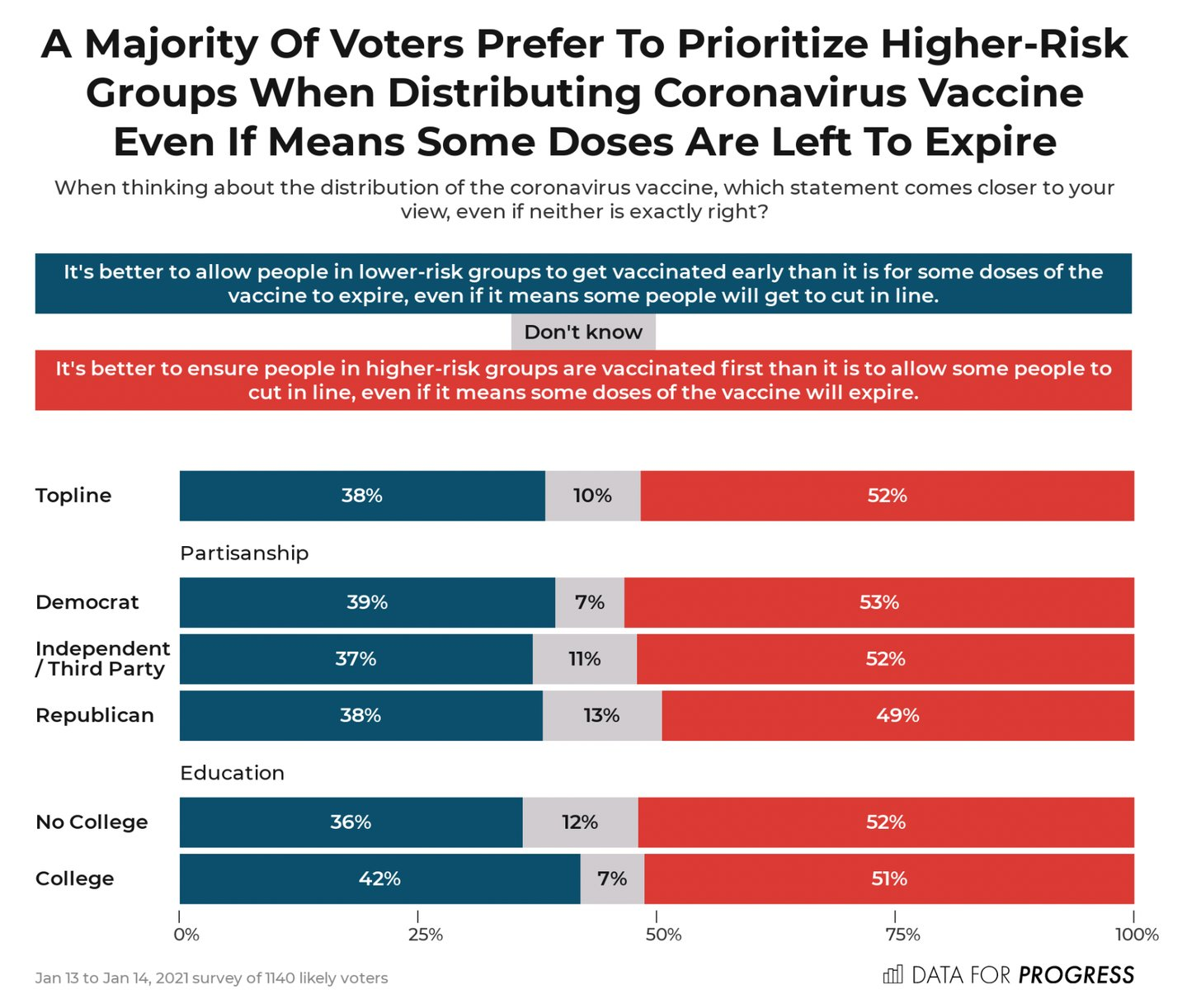
This is indeed a terrible way to ask the question and is going to warp the answer quite a bit, because it implies to people that the deserving will get their shots slower rather than faster and highlights the frame that this is somehow “cheating,” but yes a lot of people really would rather throw a dose away than let someone “cut the line” to get it. You have two cows, someone else deserves the cows more, so we should kill the cows (from a subscriber-only SlowBoring):
Not Covid-19 and I mentioned this a few weeks ago, but seriously, Matt Levine is on liquid fire and you should subscribe to his newsletter.
Sometimes people lie about their health status if you give them incentive to do so, in this case faking negative tests in order to travel.
I will not suggest allocation by scarce resources by price. I will not suggest allocation of scarce resources by price.
Once again, a reminder that we could still spend that five billion, and at the minimum do immense good in the third world. Call your local effective altruist.
Periodic reminder that we could win now if we used a sufficient quantity of rapid tests, and that the entire pandemic continues to be the fault of FDA regulations. A standalone post on rapid tests should arrive at some point in the coming week, most but not all of which you should know already.
If you fly a private plane into an isolated indigenous village, then lie about who you are and your eligibility to get a vaccine dose, being fined less than the cost of the plane trip for doing so is not going to be much of a deterrent.
Experts say serology tests unreliable, as immunity doesn’t require antibodies. What I love about this is that they’re unreliable because of false negatives, and they underestimate immunity. Which “experts” are now able to point out, because it’s now an argument against doing the obviously correct and useful thing of figuring out who is immune. Whereas, seriously, who thinks we shouldn’t use the best immunity passport test we have if that test has some false negatives? So what?
Oh, and Scott Alexander is back! Woo-hoo!
(While Scott’s return is excellent, a hit piece might still be published and the whole thing was pretty awful, so the ghosting of the New York Times will continue for now, until morale improves or Scott sends me a one-line email telling me to stop, as per my interpretation of Scott’s explanation of events, and we’ll see what happens)
The CDC Should Know This Already
We’ll be on top of this face mask thing any day now, really:
The CDC did manage this week to fix its crazy overestimate of the true number of Covid-19 cases (CDC link):
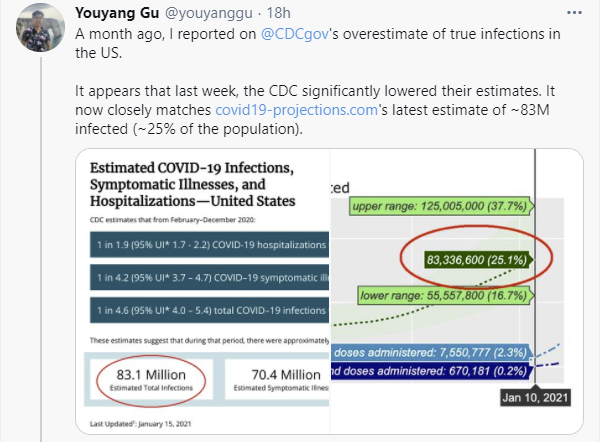
Which is great, and qualifies under the policy of always praising when mistakes are fixed rather than using it as an excuse to harp on those mistakes more, but the lack of a new released methodology is still kinda suspicious (link to paper):
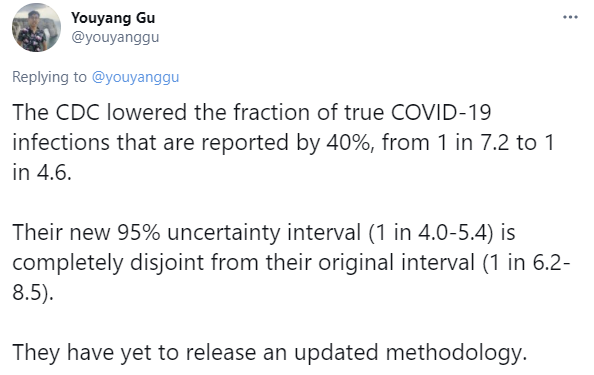

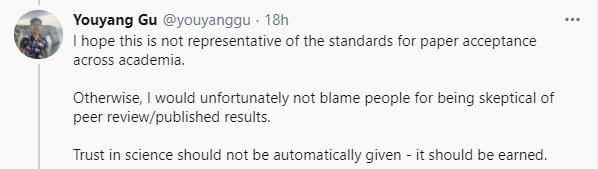
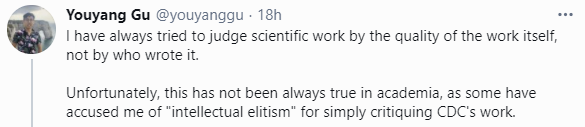
I believe Youyang Gu is going to be disappointed. The (good?) news is it seems likely the CDC essentially copied him. Hopefully he does not lose hope.
CDC admits that mixing Pfizer and Moderna vaccines is acceptable in ‘exceptional cases,’ continues to insist they are technically not interchangeable. Also admitted up to a six week wait between doses is fine.
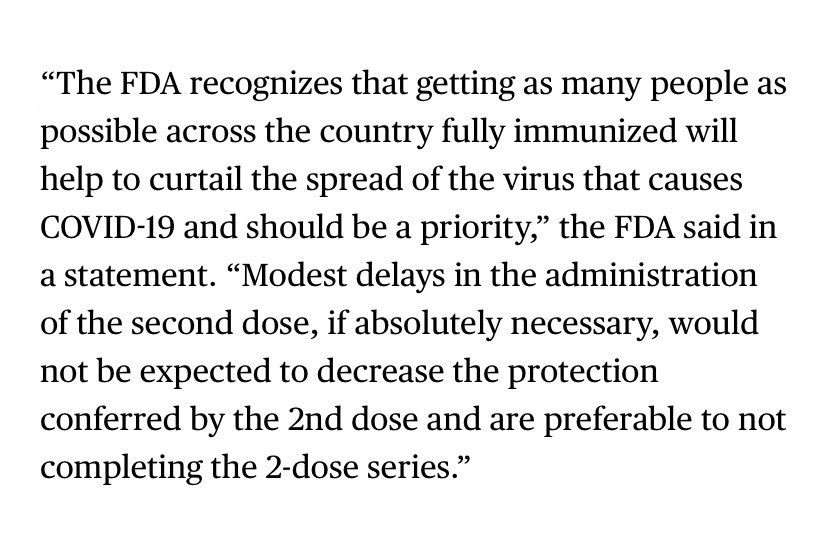
FDA should also know this already, and also eases up its guidelines on second dose timing exactly when it becomes logistically necessary to do that. Not that it contains information anyone would have doubted:
In Other News
I had a section on Bill Gates and his efforts to accelerate vaccine production, after several commenters responded to my ‘someone should help accelerate production’ by asking about Bill Gates. It got long and stands on its own so I turned it into its own post.
Malcolm Ocean updates us on the situation in Canada.
Oklahoma’s governor bought a $2mm stockpile of HCQ back when it was being touted, and is still trying to return it. Presumably it can eventually be used for its original intended purpose, it’s still a good drug people use for real problems.
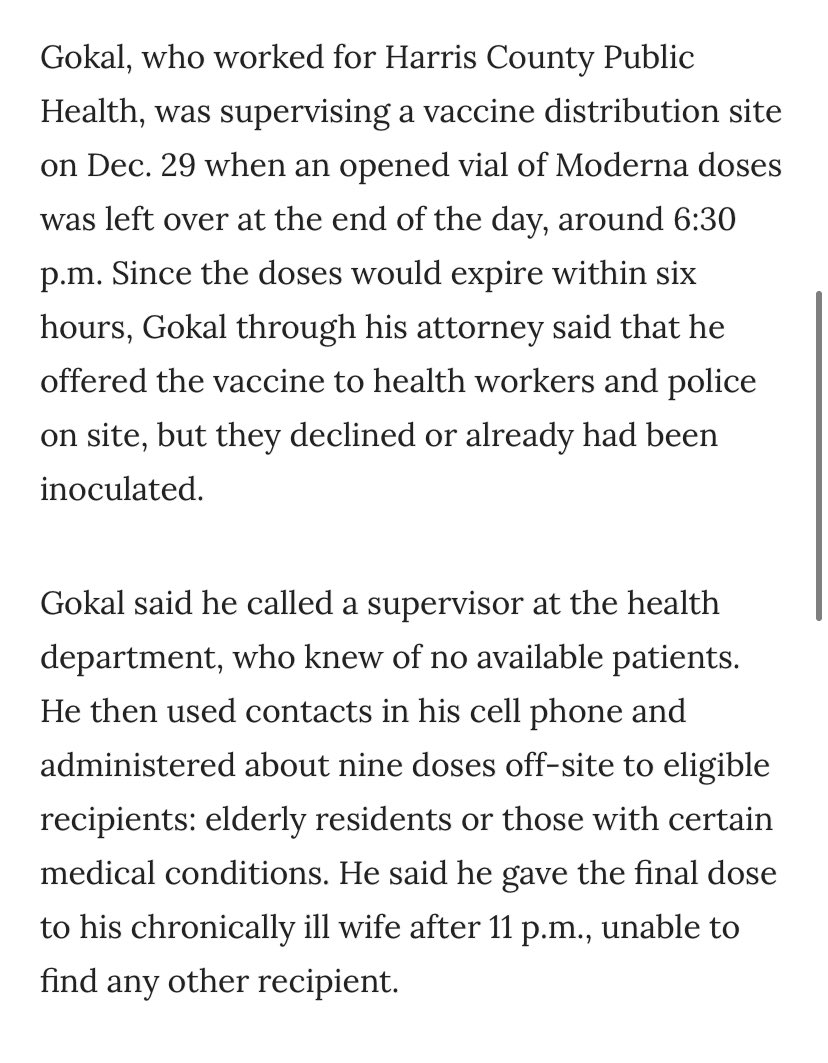
Competition for being The Worst is always intense. Consider the latest entry, a Harris County DA who (I am assuming Gokal’s account is accurate) literally arrested a doctor for stealing vaccines when he took otherwise expiring doses and gave them to whoever he could find:
Budweiser, the consensus Worst Beer, is giving up the one good thing about the brand, its Super Bowl advertising (remember the Bud Bowl? So good, chef’s kiss), and instead donating the funds to Covid-19 vaccine awareness efforts. Lack of awareness does not seem to me to be a bottleneck, but corporate virtue signaling is still expected to be good business – Budweiser officially says this will be “good for the brand.”
The WHO also ups its game to stay in competition to be the worst, taking the classic “no evidence” line rather explicitly to deny life saving medicine to pregnant women, as in and I quote “there is no reason to think there could be a problem” but still, don’t do it:

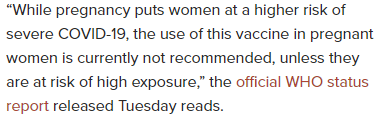

It also made the move of ‘don’t provide any word on Moderna until the end of January” which you have to admit is a strong move in this competition.
Lilly’s monoclonal antibody treatment appears highly effective in small study, says Lilly. Effect is big enough that it’s either real and the treatment is great, or it’s fraud.
First we turned to Starbucks, but that’s old and busted, so next we turned to Chick-fil-A to solve our drive-through congestion issues. Call the pros, indeed.

Luckily the judge not only dismissed the charges but yelled at the DA for bringing them. Gokal deserves a medal. At minimum, he deserves his job back.
Neat but not all that useful visual view of Metaculus forecasts about Covid-19.
Marginal Revolution links to this thread about an outbreak in Peru. Takeaways seem to be that 30-40% seropositivity does not always prevent subsequent infection waves, and that big enough waves can get to 70%+ seropositivity, with a lot of excess death.
I am strongly in favor of experimentation in general but I’m going to make an exception and say that we’d all be better off if Pfizer didn’t test its vaccine in children ages 12-15. When I heard about this, my thought was ‘no one would be so foolish as to want to prioritize children who can’t even get sick’ but no, actually, lots of people are exactly that foolish slash selfish and are ready to demand that their precious snowflakes get the protection they need ahead of others who can actually be harmed. And in fact Israel is expanding its vaccination efforts to 16-18 year olds right now. So it’s a vital line in our defense that we can claim that we don’t know the vaccine works in children, and it would be a shame to lose that defense until our vaccine supplies are adequate. Hopefully we can string this study along until then.

California continues to make strange decisions regarding its lockdown procedures, lifting regional stay-at-home orders that encompassed 90%+ of their population on Monday. All hail the control system. Things in California do not seem to be going sufficiently well that, given you’d instituted such an order, it would make sense to lift it unless your priorities (and perhaps something else that isn’t the level of infections) had suddenly changed.
You, on the other hand, have been reading this column for many weeks. So you shouldn’t be.
Israel is vaccinating 16-18 year olds because they want to protect them during high school matriculation exams which are supposed to happen starting in a few months. That's the rationale that was given when the policy was announced, at least. Also they're close to being done with every one else who wants a vaccine. Official policy is currently that people 35 and older can make a vaccination appointment, but even younger people can fairly easily get vaccinated if they want to.