Epistemic status: Speculative pattern-matching based on public information.
In 2023, Gwern published an excellent analysis suggesting Elon Musk exhibits behavioral patterns consistent with bipolar II disorder. The evidence was compelling: cycles of intense productivity followed by periods of withdrawal, risk-taking behavior (like crashing an uninsured McLaren), reduced sleep requirements during "up" phases, and self-reported "great highs, terrible lows."
Gwern's analysis stopped short of suggesting bipolar I disorder, which requires full manic episodes rather than the hypomania characteristic of bipolar II. This distinction isn't merely academic—it represents different risk profiles, treatment approaches, and progression patterns.
Now, I'm beginning to wonder: are we witnessing a potential transition from bipolar II to bipolar I? To be clear, I'm not claiming this has happened, but rather exploring whether the probability of such a transition appears to be increasing based on risk factor analysis.
(Disclaimer: I recognize the limitations of armchair diagnosis, especially of public figures. But there's value in examining these patterns as case studies in how psychiatric conditions manifest in high-functioning individuals, particularly when those individuals have publicly acknowledged aspects of their mental health. Think of this as an intellectual exercise in applied psychiatry rather than a definitive claim about Musk's mental state.)
II. The Bipolar Spectrum: A Brief Primer on Category Boundaries
Before diving deeper, let's establish some conceptual clarity around bipolar disorders.
Bipolar II involves:
- Major depressive episodes
- At least one hypomanic episode (elevated mood/energy lasting 4+ days)
- No history of manic episodes
Bipolar I requires:
- At least one manic episode (severely elevated mood/energy lasting 7+ days or requiring hospitalization)
- May or may not include depressive episodes
- Often includes psychotic features during mania
The key distinction is that hypomania, while problematic, is often productive and doesn't cause severe impairment. Mania, conversely, significantly disrupts functioning and more often comes with psychotic features.
A single manic episode automatically reclassifies someone from bipolar II to bipolar I.
III. Revisiting Gwern's Analysis: The Case for Bipolar II
Gwern's analysis presented multiple lines of evidence suggesting Musk fits the bipolar II profile:
- Musk's own statements, like his 2017 tweet: "The reality is great highs, terrible lows and unrelenting stress," followed by "yeah" when directly asked if he was bipolar, though he added "Maybe not medically tho" (a common hedge among high-functioning individuals who recognize their patterns but resist formal diagnosis).
- Work patterns showing intense productivity cycles—what Isaacson's biography called "demon mode"—followed by withdrawal.
- Risk-taking behavior both personally (the uninsured McLaren incident) and professionally (betting Tesla's future multiple times).
- Sleep patterns of 4-6 hours per night during productive periods.
- Mood oscillations between exceptional generosity and harsh criticism.
These indicators align well with bipolar II's profile: productive hypomanic episodes alternating with depressive periods, without crossing into full mania's territory.
But what determines whether someone might experience that first manic episode. Let's try risk factor analysis.
IV. Risk Factors for Bipolar Escalation: A Quantified Assessment
I've made AIs review the literature on factors that increase the likelihood of hypomanic escalation to mania. Here's how they might apply to Musk, scored by AIs 1-10 based on publicly available information as of March 2025. (The scoring system is an original creation, based on a synthesis of research findings, with higher scores indicating greater risk contribution.)
Ketamine Use (6/10)
Musk has acknowledged using prescription ketamine for depression—"a small amount every other week" according to CNN reporting in 2024. Previously, media reported on his history with recreational substances including LSD and cocaine.
While ketamine has shown promise as a depression treatment, it's a complex compound. At therapeutic doses, it typically functions as a CNS depressant, which wouldn't directly trigger mania. However, recreational use or irregular dosing could potentially destabilize mood regulation systems. Recent patterns beyond the "every other week" report remain unclear.
(An interesting connection: ketamine's mode of action involves NMDA receptor antagonism and downstream effects on glutamate systems. These same systems are targeted by lithium and lamotrigine, standard treatments for bipolar disorder. This suggests ketamine is interacting with precisely the neurochemical systems already potentially dysregulated in someone with bipolar tendencies.)
Medication Effects (4/10)
Beyond ketamine, Musk has relied on Ambien for sleep (Business Insider, 2018) and reportedly uses Wegovy for weight management. Neither medication falls into the high-risk category for mania induction like SSRIs or corticosteroids might.
However, there's potential for interaction effects. Ambien combined with ketamine could potentially amplify CNS depression, creating a rebound effect when both medications wear off. This pattern of artificial suppression followed by rebound can hypothetically destabilize mood regulation.
The risk here doesn't appear severe without evidence of antidepressant use, but medication interactions remain a relevant consideration.
Sleep Disruption (8/10)
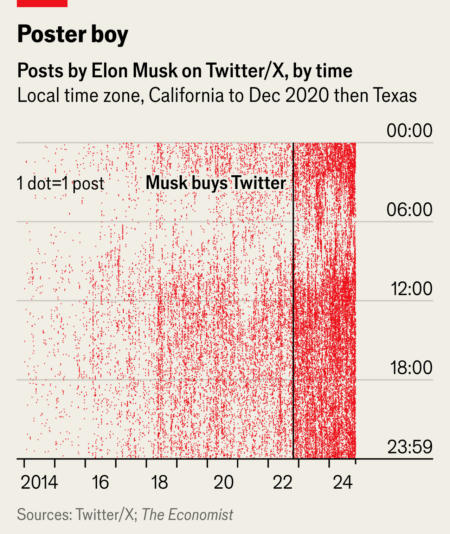
This is where the alarm bells start ringing loudly. Musk's sleep patterns are notoriously minimal—4-6 hours per night during normal periods, with reports of multiple consecutive nights with just 2-3 hours during critical project phases (per Isaacson). Basen on X posts, this seems getting more extreme.
The relationship between sleep disruption and mania is one of the more robust findings in bipolar research (Jackson A et al 2003, Wehr TA et al)
Musk's reliance on Ambien suggests he recognized this vulnerability but addressed it pharmacologically rather than behaviorally. This approach carries its own risks—Ambien's effectiveness diminishes over time, potentially leading to periods of rebound insomnia that further destabilize sleep architecture.
Given the strength of this risk factor in the literature and Musk's documented sleep patterns, this scores high on our risk assessment.
Stress (9/10)
Not much explanation needed.
Biological Vulnerability (5/10)
Musk's self-speculation about bipolar tendencies and his confirmed Asperger's diagnosis suggest a baseline neuropsychiatric vulnerability. These conditions frequently co-occur, and shared genetic risk factors have been identified.
V. Epistemic Deterioration: The Cognitive Signature of Approaching Mania
There is no public evidence of Musk experiencing a full manic episode as of this writing—no reports of psychosis or week-long periods of severely disrupted functioning have emerged. However, the continuum between hypomania and mania deserves closer examination, particularly regarding its effects on cognition and belief formation.
The DSM-5 may draw a bright line between them (mainly for insurance reimbursement and treatment protocol purposes), but neurochemically, the transition is gradual.
Perhaps the most concerning aspect of potential manic transition in Musk isn't the behavioral manifestations but the cognitive ones—specifically, epistemic deterioration. Progressive degradation of reality-testing and belief formation, leading to delusions.
For Musk, already known for bold claims this could manifest as:
- Doubling down on improbable forecasts even in the face of contradictory evidence.
- Dismissing critical feedback as fundamentally misguided. Musk's response to critics has shifted from technical rebuttals to increasingly ad hominem dismissals
- Theory of mind degradation
- Misinterpreting signals or criticism as personal vendettas. The neurochemical systems that regulate both mood and pattern recognition overlap substantially. As these systems dysregulate, coincidental events start appearing causally connected—the foundation of conspiratorial thinking.
Delusion Risk
In extreme cases, epistemic deterioration can progress to delusions—fixed beliefs resistant to contradictory evidence. Manic delusions typically manifest as inflated self-belief, imagining oneself uniquely destined or possessing special powers.
(It's worth noting that this isn't a binary "rational/irrational" distinction. The most dangerous epistemic deterioration often involves kernels of genuine insight embedded within increasingly tenuous reasoning. This is what makes the phenomenon so difficult to address, especially in genuinely brilliant people.)
VI. The Optimum of the Parabola
Creativity and productivity in bipolar spectrum conditions follow what we might call a "Yerkes-Dodson parabola"—performance increases with arousal/energy up to an optimal point, then declines as systems become dysregulated. The most productive state is often at the upper edge of hypomania, just before the transition to mania begins. It's like driving a car at maximum safe speed—fast progress, but also the point where the tiniest mistake can send you off the road.
Are we, then, watching in real-time as one of our era's most consequential minds veers toward that ditch?
This text was written by a cyborg team and re-written using AI for multiple reasons. Published anonymously mostly due to perceived risk of angry mobs.
Why do people even think this - because of his politics?