Flock – work in public with friends (beta testers wanted)
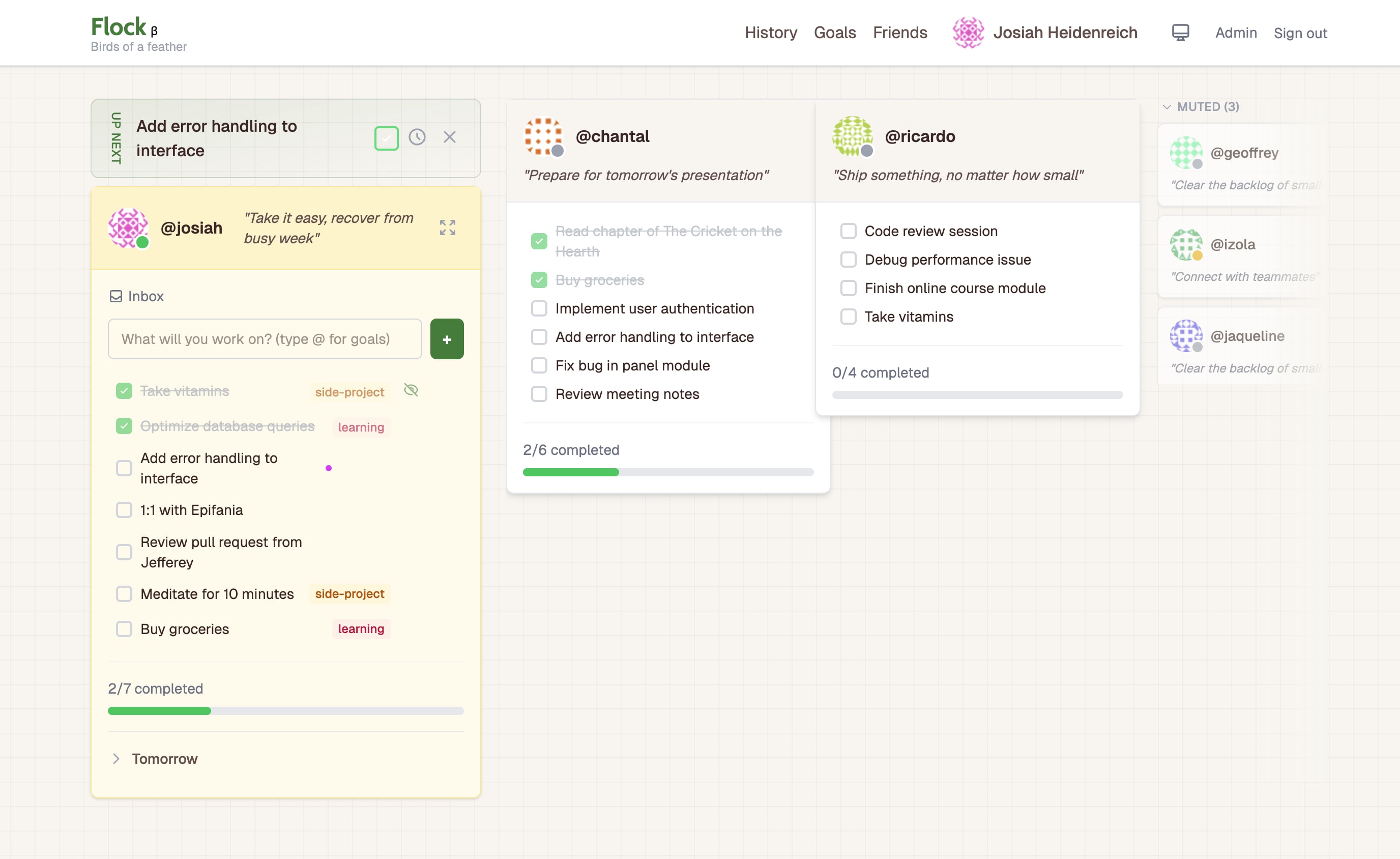
It's motivating to work alongside others—but hard to do if you're working independently. Flock lets you share your todo list with friends so you can see what each other is working on in real-time. The basic idea: you manage your daily tasks, set an intention for the day, and see...
Dec 11, 20254
I've sometimes wondered if what can loosely be called "pickup" or "daygame" (read: talking to strangers in the day to strike up romantic connections with them) might be anti-depressive. My instinct is that you need to be in a good mood first to attempt such a thing but it's possible it's actually a big mood booster – even just offering someone a compliment and moving on.