I wondered what "processed meat" means exactly and looked it up in one of the studies:
“Red meat” was defined as unprocessed meat from beef, hamburgers, lamb, pork, or game and excluding poultry, fish, or egg; “processed meat” was defined as any meat preserved by smoking, curing, or salting or addition of chemical preservatives, such as bacon, salami, sausages, hot dogs, or processed deli or luncheon meats, and excluding fish or eggs; and “total meat” was defined as the total of these 2 categories.
I also looked up "resistance training," but it is not clear exactly what is meant, and I have to assume that it is strength training.
I recommend adding this post to the boring advice repository.
Where I've heard the term used, it'd be unprocessed. As someone who can't eat the usual meat preservatives at all for health reasons, I can tell you for sure that typical plastic wrapped hamburger meat isn't preserved with anything (which, based on the examples, would probably be the reason why processed meat is bad for you).
This is good stuff!
One addition I would make to your "sleep" section: between 5% and 10% of Americans have moderate or severe sleep apnea, mostly undiagnosed. Untreated sleep apnea more than doubles mortality through a combination of cardiac problems, stroke, and maybe a cancer-promoting effect as well. There are well-known effective treatments for sleep apnea and it is kind of dumb not to get them.
The main symptoms of sleep apnea are excessive snoring, and feeling very tired during the day even if you slept a normal amount the night before. It is most common in obese and older people but sometimes happens in normal-weight and younger people as well. If you think you might have this condition, probably your highest-priority longevity intervention (after quitting smoking, if you do that) is to go to your doctor and get it checked out.
Update: I had some trouble with the app the first two nights (it stops recording if you exit it in any way), but I have audio evidence that I snore now (I don't know what counts as excessive). Time to go see a doctor about a diagnosis.
Over the last year I have become dramatically better at instilling habits in myself. I posit two main reasons for this. The first is understanding the habit formation process, as summarized by Kaj Sotala here. The second is learning to create plans that are more robust against random failure. I used to model myself as a coherent agent with some set amount of willpower to expend on the various things I found unpleasant. More recently, I model myself as a bunch of sub-agents with different goals. The subagent that tends to make plans for what I’m going to do this week is NOT the same sub-agent that will actually have to do these things. So now I make plans that can take into account a low motivation sub-agent being in charge. Sometimes this is as simple as a part of your plan that says “IF you don’t want to go to the gym THEN you will go to the gym anyway.” Yes, seriously. Sometimes it is making the activation costs of a particular action easier by removing friction from your process. Sometimes it is modeling my future self as an idiot who can’t stop eating cookies and doing things like preemptively throwing cookies away.
How would I actually go about forming a new habit? Let’s use fl...
Judging from the votes and quality couldn't this go to Main? At least with minimum further streamlining?
And if not why not?
On eating more fish: How worried should I be about mercury poisoning? Is it worthwhile to carefully select fish for low mercury content?
For instance, one guy on /r/fitness reports that 2 cans of chunk light tuna a day gave him mercury poisoning; while you're not recommending that much fish, I'd expect that health detriments appear long before full-blown mercury poisoning.
(I'm not expecting you in particular to tell me this, I just want to know if someone on LW has already done this research.)
The health benefits of fish outweight the health detriments of mercury until way beyond the level of consumption you're likely to get to.
Supporting data..?
Sunlight leads to less cardiovascular disease. (nitric oxide)
Sunlight leads to less cardiovascular disease Vitamin D.
And see if you can have someone in your life who can advocate for you in medical matters if you're not in good enough shape to advocate for yourself. (Anyone know if deeply incompetent medical care is as bad a problem in countries which aren't the US?)
(edited to add sources) (edited to add music-nerdery)
Reviewing my notes from Wiseman, I can add the following recommendations for stress:
*Listen to classical music. Actually, if you check the study, only major, baroque music was helpful. I recommend the Brandenburg concerti.
*Spend at least 30 minutes outside on warm, sunny days.
*Laugh at least 15 minutes a day.
*Source: Music can facilitate blood pressure recovery from stress.
*Source: A warm heart and a clear head. The contingent effects of weather on mood and cognition.
*Source The Effect of Mirthful Laughter on the Human Cardiovascular System
(background: I've trained in classical cello for 11 years. What follows has an inferential distance of 1 for me, and an inferential distance of quite a lot for a layperson. You should probably move along)
If you check out the music study, you'll notice that it talks about "classical" music, while I'm specifying "major, baroque". Here's why.
Classical and baroque music are different. Colloquially, "classical" refers to old music that typically gets played by v...
Usually I'm content to just lurk and read interesting posts, but here there's finally something well enough into my area of expertise that it worth making an account to contribute to!
The e-cig linked as a suggestion is a (low end, generously speaking) clearomizer system. There's nothing wrong with that, they will work as advertised and be less harmful than tobacco and all that good stuff. And if you're buying e-cigs en masse to hand out to smoker friends you can't beat the price. But it's a bit misleading to say one of these alone will add an arbitrary number of years to a persons life. The heating coils in any kind of ecig don't last forever, and low end devices like the one in the OP tend not to be disassemble-able/customizable. At $5, tossing it out and getting a new one is no big deal, really. But still.
A former smoker with disposable income (read: anyone who could afford to sustain their own tobacco habit in the first place) that's just a bit pickier would get more mileage out of a rebuildable atomizer based mechanical mod system, even a lowerish end one. It'll cost more since you'll have to buy parts individually (think building your own computer), but the increased quality o...
No. If you are a vegetarian for moral reasons consider how your personal consumption impacts suffering on the margin and maybe consider at least drinking milk.
I have experienced consequences of donating blood too often.The blood donation places check your hemoglobin, but I have experienced iron deficiency symptoms when my hemoglobin was normal and my serum ferritin was low. The symptoms were twitchy legs when I was trying to sleep and insomnia, and iron deficiency was confirmed with a ferritin test. The iron deficiency symptoms went away and ferritin went back to normal when I took iron supplements and stopped donating blood, and I stopped the iron supplements after the normal ferritin test.
The blood donation pl...
I don’t care if you start with an exercise habit of one pushup a week, but you must do something.
Beeminder Beeminder Beeminder. Having an email reminder to exercise, and a penalty for not doing so, has been tremendously helpful for me- I now actually lift weights three times a week, as compared to just when I remembered to do so on my own.
I notice that I am confused about what makes a post worthy of being Promoted. This post is well-researched and has an incredibly high score and lots of interesting comments. Is it that MIRI/CFAR/et al are afraid that someone might implement these and later sue if they don't get results, or somerthing?
As it is, Main but not Promoted is currently the least visible location on the site.
Well, I was surprised by the flossing claim, looked it up and found a correlational study with control variables. Give me my choice of control variables in a correlational study and I will prove that smoking cigarettes prevents lung cancer. And I was a bit worried about other items listed even before then. So I decided not to promote.
Great article. Lots of really good information. A few questions:
Well it turns out that fish oil pills suck, and you’d need to take approximately 9 times as much to have the same effect as eating fish, at which point they’d have dangerous blood thinning effects.
Does anyone have a link to this full study? I'd like to see the full data. The abstract is confusing. It says you would need " two- and ninefold higher doses of EPA and DHA, respectively, if administered with capsules rather than salmon," but it's not clear which numbers you need ...
Regarding driving safety: A couple of years ago I asked my old driving instructor if he knew of a good book on driving safety I could use to increase my skills. He pointed me to some of Fred Mottola's guides at the National Institute for Driver Behavior. I ordered pretty much all of the reading / course material he has available, and I thought they were excellent. There's a lot of little tips for marginally increasing safety, and he focuses a lot on developing good habits so it doesn't require constant vigilance.
In order to get the full benefits of his pro...
Get tape and cover lights. Try orange glasses to prevent blue light from destroying your endogenous melatonin production after 10pm.
I have always been confused about this one part. Seems like this is the place to ask, for once.
Where do these exact o'clock figures always come from when people are talking about sleep optimizing?
I mean, 10pm by which clock? Certainly, the position of arrows on my watches does not influence melatonin production. Is it calibrated by amount of daylight? But in the area I live in, 10pm can be a middle of the night or not-even-...
I'm very surprised that there is no mention of a low-dose aspirin regime here. Low dose aspirin can greatly reduce chances of stroke, heart attack, and cancer. The main caveat is that there is increased chance of bleeding or stomach ulcer, the latter of which can be avoided by taking with food.
I looked into the numbers and it's a wash for people under 45. The risks are greater than often presented, likely because the marketing is targeted at people at heightened risk who really do need to be convinced to take it.
Examine.com is much less positive about CoQ10 writing "all the noticeable effects (more vitality) could potentially be placebo. It is very much a faith buy and the costs if you take it in the wrong manner (without a fatty transport) could be quite high financially."
I was pretty surprised about blood donation. My intuition is screaming that it must be one of those correlation/causation things where unhealthy people are discouraged from donating blood, but on the other hand, the researchers are all surely very well aware of this issue and must have taken steps to correct for it.
Anyway, have you thought about typically sub-clinical viruses like cytomegalovirus? I recall reading that a CMV infection cuts a few years from your life expectancy. I don't have research to back it up, but I think it's a good idea to avoid having intimate contact (e.g. casual sex) with lots of people.
I was pretty surprised about blood donation.
Males tend to have iron overload which is bad for you. The easiest way to fix it is to bleed on a regular basis.
Women don't have that problem.
Those of us disqualified from donating blood should probably try to get into some form of exercise that involves a lot of blood loss; like skateboarding over sharp rocks, fencing with un-foiled blades, or taunting apex predators in their natural habitat. A new Ev-psych explanation for why men engage in this sort of activity more than women!
I imagine it'd be rather difficult to find a hobby that reliably takes a pint of blood a year and doesn't kill or seriously injure you.
Pet leeches :-P
Also relevant to longevity are supplements for reducing the cognitive decline that comes with aging, such as piracetam.
Why should we listen to you and not, say, the Harvard School of Public Health ?
That is, why do you think you did a better job of reading and interpreting the literature and publishing guidelines?
Regarding sleep temperature, I've seen contradictory recommendations.
This article references a finding that "finding that facial warming helps send people to sleep". And Wikipedia writes
Some of the few factors known to increase slow-wave sleep in the sleep period that follows them include body heating (as by immersion in a hot tub)...
Though, this guy writes
..."A hot bath will increase your skin temperature, which eventually decreases your core body temperature. Do the same thing for yourself that you’d do for a young child—make sure you
On the topic of whether it's useful to worry about longevity when you're young: I just saw this article in the NY Times, which suggests that it is.
Ovo-lacto vegetarians live significantly longer than vegans
Where does it say that the difference is significant? The only mention of this I see in the cited paper is table 7, and the CIs there overlap a great deal. (And it goes on to say that the numbers should be "interpreted with caution because of the uncertainty of the dietary classification of subjects in the Health Food Shoppers Study".)
Interesting that there is not much discussion in the comments about weight loss, which is very hard as we all know. And not much discussion about cholesterol either for some reason.
I would just like to point out that Body Mass Index and cholesterol are not very good predictors of risk and that there is some evidence that waist/hip ratio may be a better metric to track.
I clicked through to your recommendation to floss and saw an associational study with a set of control variables. This is such a horribly bad sign that it makes me doubt the rest of your post.
Floss does have the weakest evidence going for it, hence its position last on the list. It stayed above the "worth it" line due to the low cost and risk. I also believe it has an impact on quality of life even if the mortality effect turns out to be small. I do need to add a discussion of this to my post at some point.
By the way, it seems to me that we need to think in more detail about the relationship between happiness and stress. For example, I have pretty high-stress job (I am a litigation attorney) but at the same time it's a lot of fun most of the time and I am reasonably happy with it. How many more years could I expect to live if I were a trust fund baby?
A few studies have been done on the relationship between retirement age and longevity. As I recall, the best studies seem to show little or no relationship once you eliminate consideration of individuals wh...
The ToC makes it looks like "blood donations" and "exercise" are among "things that will eventually kill you"...
Changing bed cloth once a week.
This recommendation is not in the list and I heard about it the first time just now:
Huffington Post: This Is What Happens If You Don't Change Your Bed Sheets (And how often the average person actually does it.)
I can't vouch for it but the potentially long list of benefits - and the long time you spend in bed - same as the arguments for mattresses - make this a potentially high-value intervention.
Buying an e-cig for yourself or people you know who smoke are possibly the single cheapest intervention for adding years to life. E-cigs have very high success rates in getting people to quit smoking and are absurdly cheap. You can spend under $10 and add 14 years to someone’s life. I buy them just to give away.
I have bought such an e-cig and gave it to a friend. It was received positively. It also prompted a discussion about the (unknown?) effects of e-cigs. Even though this was only cited as an often given counter-argument I nontheless wonder what the research behind e-cigs shows? Can you provide references that back your claim of getting people to quit?
How much have you looked into potential confounders for these things? With the processed meat thing in particular, I've wondered what could be so bad about processing meat, and if this could be one of those things where education and wealth are correlated with health, so if wealthy, well-educated people start doing something, it becomes correlated with health too. In that particular case, it would be a case of processed meat being cheap, and therefore eaten by poor people more, while steak tends to be expensive.
(This may be totally wrong, but it seems like an important concern to have investigated.)
Ok, so basically, I need to floss more and drive less recklessly (when I drive at all, which is rarely). But other than that, I'm doing good at targeting longevity.
steeples fingers
Eeeeexcellent. Everyone who claims to aim for immortality or personal happiness but doesn't exercise, turn in your rationality card right now.
I can't claim any super-insightful techniques for actually building good habits and making good decisions, personally. My main technique is just to make a decision by putting myself in the shoes of future-me and asking what he's going to care about more.
This is a useful post. Thank you for writing it.
You claim that "Eggs and whole milk are very nutrient dense." I think that's quite a controversial statement. Here are the nutrition facts for 100 Calories of whole milk and spinach:
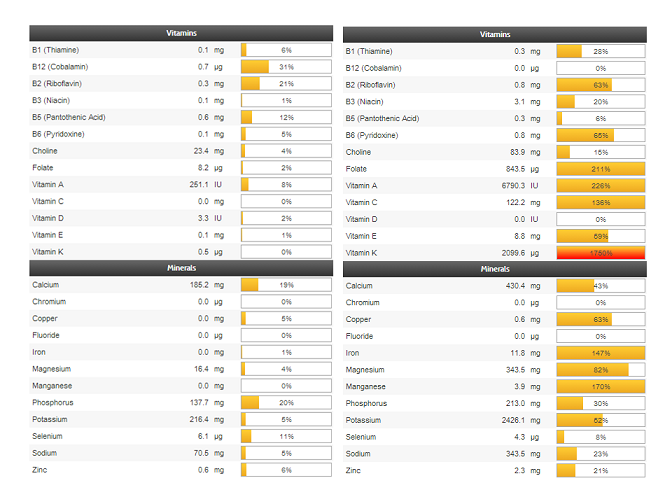
I've downvoted your post due to use of a misleading graphic (EDIT: Downvote retracted after your reply). The graphic is comparing low fat milk, not whole milk, while whole milk has much more nutrition than low fat milk. Additionally, nutrient density can refer to both nutrients/calorie, nutrients/volume, and nutrients/price. All are important measures. Spinach wins on nutrients/calorie, but the other two, not so much.
Whole milk, for example, has 124IU of Vitamin D while the chart only lists 2.4 IU, which approximates the 1% fat figure from Google's nutrition information.
This is what 200 calories of whole milk looks like. This is 200 calories of eggs. This is 100 calories of spinach.
{kind=link}
{kind=link}
{kind=link}
Spinach has little protein (0.9g/serving), while eggs and milk both contain 8g and 7g per serving. This extremely important number is missing from the chart. A cup (30g) of spinach (standard serving size) contains 7 calories, so you'd need to multiply your numbers in the charts by 0.07 to get the expected nutrition per serving of spinach. A serving of whole milk (8oz/244g) is around 148 calories, so we'd need to multipy by 1.48 for a serving:serving comparison. Doing this, the differences in nutrient c...
I wonder if farmed salmon, presumably full of colors and antibiotics, has the same beneficial effect as wild.
A quick google search indicates that salmon farming has become much better in recent years, and might surpass wild salmon soon. Most of the information on fatty acid profiles that I can find is from 2008, before these advances. The chart on this page indicates that farmed salmon has much more fat with a smaller proportion of omega-3. The total n-3 is close (1.8g farmed vs 1.7g wild), but if most of the extra fat is n-6, then you're not doing much for fixing the 3:6 ratio.
What do you think of the health effects of too much sitting? That seems to be a hot topic recently. http://www.mayoclinic.org/sitting/expert-answers/faq-20058005
I missed a section on sugar (even if it just says that this is not covered or e.g. link to http://lesswrong.com/lw/je5/critiquing_gary_taubes_part_3_did_the_us/ )
ADDED: And a sentance about caffeine.
Very good post.
How I plan to act on it:
reduce processed meat further (but not unprocessed meat)
consider adding some restance training to my exercise (once I figure out which fits best and needs no weights etc.; probably http://en.wikipedia.org/wiki/Bodyweight_exercise )
check my blood measures with you info in mind
consider yearly blood donation
More exposure to sun
I already ordered an e-cig to give to an acquaintance.
Why do you think so?
It's slightly counterintuitive, but studies say that this is what happens. I'll just paste a few paragraphs from the article linked by OP:
...Tests done since 1933 show that people who talk about their intentions are less likely to make them happen.
Announcing your plans to others satisfies your self-identity just enough that you're less motivated to do the hard work needed.
In 1933, W. Mahler found that if a person announced the solution to a problem, and was acknowledged by others, it was now in the brain as a “social reality”, even if the solution hadn't actually been achieved.
NYU psychology professor Peter Gollwitzer has been studying this since his 1982 book “Symbolic Self-Completion” (pdf article here) - and recently published results of new tests in a research article, “When Intentions Go Public: Does Social Reality Widen the Intention-Behavior Gap?”
Four different tests of 63 people found that those who kept their intentions private were more likely to achieve them than those who made them public and were acknowledged by others.
Once you've told people of your intentions, it gives you a “premature sense of completeness.”
You have “identity symbols” in your b
You appear to possess some misconceptions about weight training.
they take space,
A stack of plates with the barbell stored vertically takes 0.2m^2 (~2sqft). Here's a picture of a 330lb set for demonstration; wine bottle and keyboard for scale. I have a lot more equipment than just the barbell, but that's because I do powerlifting and it's a hobby.
are no fun
This is a matter of perspective and preference. I find weight lifting to be extremely fun, especially the sport of powerlifting. Furthermore, it has no bearing on the fact that weight training is the most effective and efficient means of getting stronger.
cannot be combined with useful activity and often encourage too simple movement patterns.
The deadlift, overhead press, and row are three of the most fundamental movements a person can do. In sports science terms, these are highly general movements, which means that increasing strength in these movements will have positive carry over to every other physical pursuit that uses similar movements. Runners use the deadlift to improve their running speed, for example, and throwers use the overhead press to improve their throwing distance. Your assertion that they can't be ...
The section "How to actually form new habits" is small and doesn't fit in well. I recommend removing it or making it into a separate post or add it as a comment. There are some posts on this topic already that might be referenced roughly falling into the How To Actually Change Your Mind category.
The linked study for processed meat is a dead link, but it's on archive.org or alternatively this is a working link: https://pubmed.ncbi.nlm.nih.gov/20479151/
There is a problem with it, though. This is from the abstract:
> Conversely, processed meat intake was associated with 42% higher risk of CHD (n=5; relative risk per 50-g serving per day=1.42; 95% confidence interval, 1.07 to 1.89; P=0.04)
P=0.04 is way too high and my subjective probability for it replicating is somewhere below 50%.
Why do you think exercise improves health? Is it just an educated guess (if so, then what is the reasoning behind it), or is there actually some study establishing causality? I found https://bjsm.bmj.com/content/52/14/890 which says:
> As presented by Kujala, RCTs, the gold standard in epidemiology for inferring causality, have failed to provide conclusive evidence in this context (eg, Lifestyle Interventions and Independence for Elders,8 Look Action for Health in Diabetes,9 Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Traini...
Very nice article! Regarding the benefits of alcohol: for those curious, it is well established at this point that alcohol is actually protective against arterial plaque; it just has all sorts of other problems. This is just for kicks mostly, but I read a publication that said that for people who have ALL the following criteria:
Male (No women because alcohol increases risk of breast cancer)
...45 years Does not smoke No family history of addiction or substance abuse No personal history of addiction or substance abuse "Occasional drinker" (has a cou
As it turns out, there are actually two types of LDL,
Of course there are. For pretty much every X which is associated with human health, closer investigation will reveal that there are two types of X -- "Good X" and "Bad X."
I am considering writing a program that will launch this page in my web browser every few hours.
(While most of these interventions are things with a surprisingly high cost in terms of stress, the one I like the least but am least stressed about is the recommendation to eat more fish. I am not a fan (nor much of an enemy) of fish. I will gladly save any recommended recipes that manage to include fish and all its benefits without making it overly obvious that I'm eating fish. I could always try and self-modify so that I no longer treat fish as pretty far down the preferred meat hierarchy, but using it in something more desirable in general sounds way more fun. Bonus points if it's something well balanced.)
I praise your for the effort.
But I have one problem: how do I explain it to others? People might ask me one day "why are you doing/concerned with that?" and what my reply be? "Some guy on Lesswrong told me, but don't worry it's a rational site!"
That's silly. Instead of spreading one-dimensional awareness, you should instead spread academically correct information and let it do it's course. That way, if someone ever asks me why, I can give them a link, or at least the bottom line. Depending on how curious they are they might even read it...
Are you planning to do a post on nutrition later?
Are waterpiks as good as flossing?
It seems to be that many earlier studies claiming harm from red meat did not adequately separate out the huge effect size of processed meat.
And here I've been thinking getting the chicken sandwich at Subway or eating smoked turkey sandwich meat was healthy. [Edit: Because of this post, I will not be doing that anymore.]
But I am not really convinced that eating red meat can be healthy. It seems safer to keep it as an "occasional indulgence." Edit: That first link was not clear. Here's another.
I don't know anything about testicular cancer, but are self-exams useful for breast cancer? I know that the data argues against mammogram-everyone-annually + the ensuing unnecessary surgeries caused by not-harmful tumors or other false positives - no increase at all in life expectancy and presumably there's a significant psychological (and $) cost.
Breast self exam is not recommended by the Susan G. Komen foundation, neither recommended nor discouraged by the Memorial Sloan Kettering Cancer Center, and the National Cancer Institute reports no benefit but an increase in biopsies of benign tumors.
Testicular self-exams have not been studied enough for recommendations to be made, according to the American Cancer Society.
A word of warning about eating fish: lots of kinds of fish are contaminated by mercury. My psychiatrist ate sushi regularly and he ended up with mercury poisoning. :(
Melatonin pills work for many, but make sure you start with 75mcg (cut these into fourths), rather than the 3mg most pills come in.
Why is it important to use the lower dose? (I started using 3mg pills after reading recommendations here, and they work excellently)
Don’t publicly commit to your plan in the comments, this makes you less likely to do it
This one surprised me. It's the exact opposite of advice I've seen elsewhere here on social precommitments.
the highest plurality
Excellent post, so naturally I nitpick the language... anyway, 'plurality' means "largest fraction but not a majority". So "highest plurality" is redundant.
On the subject of exercise: What intensity are we talking about for the endurance? Is it sufficient to bicycle, or do you need to work up a lot of sweat?
There is a lot of bad science and controversy in the realm of how to have a healthy lifestyle. Every week we are bombarded with new studies conflicting older studies telling us X is good or Y is bad. Eventually we reach our psychological limit, throw up our hands, and give up. I used to do this a lot. I knew exercise was good, I knew flossing was good, and I wanted to eat better. But I never acted on any of that knowledge. I would feel guilty when I thought about this stuff and go back to what I was doing. Unsurprisingly, this didn't really cause me to make any positive lifestyle changes.
Instead of vaguely guilt-tripping you with potentially unreliable science news, this post aims to provide an overview of lifestyle interventions that have very strong evidence behind them and concrete ways to implement them.
A quick FAQ before we get started
Why should I care about longevity-promoting habits at a young age?
First, many longevity-promoting lifestyle changes will increase your quality of life in the short term. In doing this research, I found a few interventions that had shockingly large impacts on my subjective day-to-day wellness. Second, the choices you make have larger downstream effects the earlier you get started. Trying to undo years of damage and ingrained habits at an advanced age really isn’t a position you want to find yourself in. Third, extending your life matters more the more you believe in the proximity of transformative tech. If the pace of technological improvement is increasing, then adding a decade to your life may in fact be the decade that counts. Missing out on life extension tech by a few years would really suck.
Isn’t longevity mostly just genetics?
That's what I believed for a long time, but a quick trip to wikipedia tells us that only 20-30% of the variance in longevity is heritable.
What sort of benefits can I expect?
The life satisfaction of people who remain independent and active actually increases significantly with age. Mental and physical performance are strongly correlated, meaning maintaining your body will help maintain your mind. The qualitative benefits for life satisfaction of many of these interventions can be so dramatic that it is hard to estimate them. The gulf in quality of life between people maintaining good habits and those who do not widens with age.
How were these recommendations generated?/Why should I believe you?
This post summarizes studies at the intersection of having large effects, large sample sizes, and being well-designed in terms of methodology. The cutoff for an intervention being “worth it” is somewhat subjective given that there is often only a rough estimate of the overall effect sizes of various interventions in comparison to one another. CDC mortality statistics were used to determine the most likely causes of death in various age brackets. The list of things that kill people balloons significantly as you get towards the less common causes of death and I have limited research time. Individuals who face unusual health circumstances should of course be doing their own research and consulting health professionals.
This brings me to my disclaimer:
This post is not intended to diagnose, treat, cure, or prevent any disease. No claim or opinion on these pages is intended to be, nor should be construed as medical advice. Please consult with a healthcare professional before starting any diet or exercise program. None of these claims have been evaluated by the Food and Drug Administration. Suggestions herein are intended for normal healthy adults and should not be used if you are under the age of 18 or have any known medical condition.
Alright, let’s dive in.
Things that will eventually kill you
CVD
At the top of our list is cardiovascular disease, or CVD, causing the plurality of all deaths by far. We will break down the controllable components of CVD in terms of lifestyle interventions.
Smoking
This doesn’t need much of an explanation. Responsible for the majority of lung cancers, respiratory diseases, and a huge contributing factor to CVD. Buying an e-cig for yourself or people you know who smoke are possibly the single cheapest intervention for adding years to life. E-cigs have very high success rates in getting people to quit smoking and are absurdly cheap. You can spend under $10 and add 14 years to someone’s life. I buy them just to give away. Recommended products: 1, 2.
Alcohol
Some controversy over possible benefits of small amounts, but large amounts definitely bad. Avoiding alcoholism is a whole subject I won’t tackle here.
Blood Pressure
Second to tobacco in effect size. Blood pressure is one of the things most people ignore. It is extremely cheap and easy to start monitoring your blood pressure, and there are things you can do if you find it to be high. You want your blood pressure to be about 120/70. If you are higher than this there are some simple things you can do. The first is to exercise and eat fish every week, especially salmon. There are also a few supplements that have been found to be helpful.
A quick note about my criteria for inclusion for supplements: I am extremely dubious as to the benefit of most supplements. Study after study shows that most of them are a waste of time and money. The fish example given above is a good illustration. You might ask why you can’t just take fish oil pills. Well it turns out that fish oil pills suck, and you’d need to take approximately 9 times as much to have the same effect as eating fish, at which point they’d have dangerous blood thinning effects. So when I recommend a supplement it has to meet a pretty stringent list of requirements.
1. Large effect seen in multiple randomized controlled trials.
2. Therapeutic dose is a tiny fraction of the toxic dose, or no toxic dose able to be identified because it is so high.
3. Side effects comparable to placebo.
4. Dose size is commensurate with an amount it would be reasonable to ingest in natural form.
So basically I weight any downside risk very heavily given the spotty track record of the general reference class of supplements.
So what passes these criteria for blood pressure?
1. CoQ10, large effect size in multiple studies
http://www.ncbi.nlm.nih.gov/pubmed/14695924
2. Flavonoids/anthocyanins, these compounds are present in things like dark chocolate, fruits, and teas.
http://ajcn.nutrition.org/content/88/1/38.short
3. Garlic
http://www.biomedcentral.com/1471-2261/8/13/
I have personally had success lowering my blood pressure from the 140’s to the 120’s with these supplements keeping my exercise levels constant.
Blood lipids (cholesterol)
Here the conventional recommendations appear to be wrong, or at least somewhat misguided. First, some theory. Blood lipids are composed of a variety of substances, but for our purposes we will stick to the ones tested for in blood panels and how to interpret these numbers. A typical blood panel will report LDL, HDL, and Triglycerides. The simple story of “high LDL bad” does not accurately reflect risk of CVD. The most powerful predictor of CVD in terms of blood lipids is the Triglycerides to HDL ratio.[1][2][3][4][5] The higher the triglycerides and the lower the HDL, the greater the risk. This relationship holds independent of LDL levels, which are usually the focus of cholesterol discussions with health practitioners. As it turns out, there are actually two types of LDL, and distinguishing between them is something not usually performed on a blood test. The reason for the prolonged confusion arises from the correlation between a poor HDL:Triglyceride ratio and prevalence of the unhealthy type of LDL. As a result, potent cholesterol lowering drugs are over prescribed. For people with a healthy ratio of triglycerides:HDL, a total cholesterol between 200-220 (traditionally considered “high”) is actually correlated with lower mortality,[6] and aggressive lowering with drugs resulted in worse health outcomes. This is not to say that statins (cholesterol lowering drugs) are not useful. On the contrary they seem to be highly helpful for patients recovering from a cardiovascular event, but they have shown no benefit for people with no history of problems.[7] Statins have serious side effects[8] and should not be taken lightly. Be skeptical.[9]
So how does one go about lowering their triglycerides and raising their HDL? Again, exercise and eating fish are awesome here. Excessive fructose intake raises triglycerides, and this relationship is worsened by high BMI. Fiber and resistant starch from fruits, vegetables, and tubers has a positive effect. Intermittent fasting has also shown promising effects here.
BMI/Obesity
There are some controversies here I don’t really want to get into the details of as it is a complex subject. I do want to mention that health interventions should not have an excessive focus on whether one is losing weight. Many of the interventions discussed here have significant effects (for example on insulin sensitivity, c-reactive protein, and fasting blood glucose) even when body composition does not change. Getting BMI below ~27 should be a priority however, as it has wide ranging effects across all other interventions.
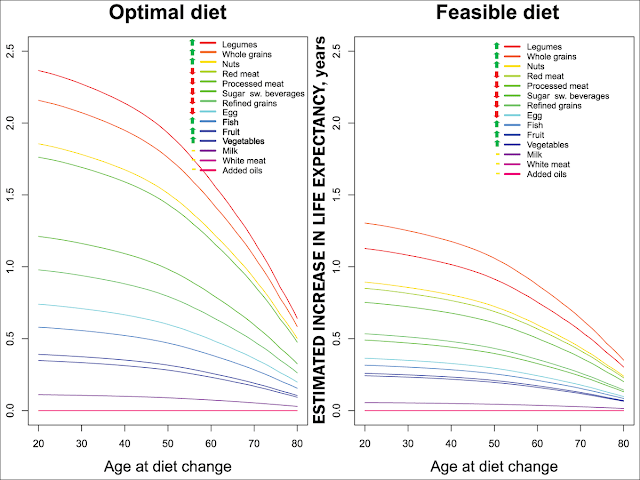
Nutrition
This is a big subject, and we’re not even going to attempt to go into detail. This section will focus on the largest high level features of a diet that have positive or negative impact. Processed meat consumption has the single largest negative effect on health. It is shockingly bad, even if you already suspected as such.[1] In contrast, a bit of red meat has actually been found to be neutral. It seems to be that many earlier studies claiming harm from red meat did not adequately separate out the huge effect size of processed meat. Fish and nut consumption appear to be a grand slam for CVD in particular and also just for overall health.[2][3] Pescetarians live significantly longer than vegans,[4] lending support to fish consumption. Outside of specific foods, common micronutrient deficiencies have been indicated in everything from cancer, to immune system suppression, to poorer physical and mental performance, to sleep problems, greater inflammation, and even depression. Really there’s too much material there to cover, there are just pages and pages of studies.
There’s also the bad news that multivitamins mostly don’t do anything. There has not been found an alternative to eating a variety of nutrient-dense whole foods. Though vitamin D supplementation appears to be quite beneficial. Another LW user, John_Maxwell_IV, and I are trying to make this easy with our startup MealSquares.
Blood donation
The studies related to this have some methodological issues but overall the effect size is so large, and the cost and risks so low, that it is worth inclusion. Several studies have indicated that, for men, regular blood donation results in a massive reduction in heart attack.[1][2][3] Other studies have found no such relation.[4] There are also additional health benefits to blood donation.[5] These are just some of the studies on this subject, but on balance after reviewing the evidence, I can say that donating blood once a year is almost certainly worth it if you're a man. Donating too often is probably bad for you though.
Exercise
This topic is large enough that I am separating out my actual recommendations into another post and purely discussing the health benefits here. Exercise is probably the single most important lifestyle intervention. Even minimal amounts of exercise have very large impacts on longevity and health. We’re talking even walking 15 minutes a day causing people to live longer. Even ignoring quality of life you are looking at a 3-7 fold return on every minute you spend exercising in extended life,[1] perhaps even exceeding that if you are making optimal use of your time. Exercise has a positive impact on pretty much everything that contributes to mortality. I don’t really know how to convince you, the reader, that the future actually exists and that future you will be incredibly angry or sad that you didn’t put in a small effort now for a better life later. But everyone has already told you this your whole life. So I’m going to contrast it with the inverse. Most of the activities that we associate with fun and leisure involve some aspect of physicality, even if it’s just walking around with friends. Losing access to these activities as can and does happen to people represents a massive decrease in quality of life. If you are reading this and you are young, you are able to simultaneously ignore your body’s need for exercise, and demand performance of it when necessary to enjoy yourself. This will not remain true forever. Exercise has a protective effect against exactly the sorts of degenerative injuries that deprive people of their freedom of movement and activity.[2] I don’t care if you start with an exercise habit of one pushup a week, but you must do something.
Let’s move on to some relevant considerations assuming you want to exercise. What sort of exercise should I be doing? Several studies have indicated that endurance athletes enjoy the greatest improvements in longevity. I would agree with this but caution that often the groups in such studies with the best health outcomes are those that do engage in resistance training as well. Soccer and other team sport players, for example, often perform resistance training as part of their overall conditioning. This seems to be overlooked because they do not perform it at the same level of intensity as athletes in the power sports. Long distance skiers and bikers also generally train lower body strength moves at an impressive level compared to the general public, even if it is a level significantly below that of power athletes (e.g. here is an example of a training regime for a competitive skier). My point is simply that you shouldn’t read a study that says “endurance athletes live longer” and assume that all you need to do is run. Strength training also has significant effects on insulin resistance, resting metabolic rate, glucose metabolism, blood pressure, hormone balance, joint health, organ reserve, depression, increases in HDL, reduction in back injuries, sleep quality, and a variety of harder-to-quantify quality of life improvements.[4][5][6][7][8] I go to the trouble to cite resistance training so heavily because I feel that the benefits of cardio are generally well-understood, but I regularly encounter the idea that resistance training is only for people who want to look like a gross bodybuilder.
Hopefully I have established that one should do both endurance and resistance training. Program specifics will be included in the other post as well as info on when benefits taper off.
Edit: Exercise post is up here.
Stress
Stress affects almost every system in your body. It increases disease risk by acting as an immunosuppressant. It directly impacts blood pressure, sleep problems, skin conditions, anxiety, depression, and even heart problems. Chronic untreated stress is often considered a causal factor in many other ailments people are medically treated for. Stress often goes untreated because alleviating it is seen as low priority. Whatever we are doing right now is worth a little stress. This can be true, but over a longer time horizon failing to learn better ways of managing stress really harms us. To confront stressors you must confront ugh fields. Non-productive coping mechanisms are the norm here: procrastination, abuse of substances including food, sleeping too much, blame as a curiosity-stopper etc. Simple strategies for dealing with low level stressors include things such as meditation, gratitude journaling, reflecting on and updating goals, or even just paying other people to deal with a recurring source of stress. Two previous LW posts have excellent advice in this area: How to Be Happy and Be Happier.
If you are depressed and don't know where to start on getting help please take a look at Things that sometimes help if you're depresed.
Supplements that impact stress include
1. Rhodiola Rosea: http://www.sciencedirect.com/science/article/pii/S0944711310002680
2. Ashwaghanda root, which shows promise for chronic anxiety: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3573577/
Sleep
Chronic insomnia is a massive source of stress for many people and poses a huge mortality risk. In one study, people who got chronically less sleep had 3 times the mortality risk as people who slept well![1] You cannot afford to not start optimizing your sleep. It is important that your sleeping place be a quiet, dark, cool environment. You can use simple methods to improve each of these parameters. Forehead cooling has shown great promise in clinical trials.[2] You can accomplish this with a gel pack that is cool (not ice). Even small LED lights in your room impact sleep quality because the melatonin production system is very fragile and sensitive to light.[3] Get tape and cover lights. Try orange glasses to prevent blue light from destroying your endogenous melatonin production after 10pm. Regularize your sleeping and eating schedules. Expose yourself to bright lights in the morning to calibrate your circadian rhythms. Afternoon/early evening exercise is beneficial in making you sleepy. Melatonin pills work for many, but make sure you start with 75mcg (cut these into fourths), rather than the 3mg most pills come in. A teaspoon of raw honey before bed helps prevent some people from waking multiple times throughout the night.
Consider reading this excellent info from Yvain on sleep apnea, especially if you snore excessively or feel very tired even after a full night's sleep.
Cancer
Almost all of the risk factors for cancer have some overlap with CVD, meaning most of the advice above works for cancer too, but there are a few additional considerations worth discussing.
Cancer and UV exposure
One of the surprising results of my research was that conventional wisdom appears to be wrong here. There is not a simple relationship between UV exposure and increased cancers. Specifically, while increased sunlight exposure is correlated with higher incidence of skin cancer, it appears that it is also correlated with a decreased risk of 5 other cancers that are far less survivable.[1] This is a straightforward trade off, getting sun exposure wins by quite a lot. Shade your face to avoid photodamage to your skin and macular degeneration of your eyes.
Breast cancer and testicular cancer
Redacted, see Vaniver's comment here.
Floss
No, seriously. Not flossing is way more lethal than you think.[1] You should also see a dentist regularly, even if you have to pay for your own insurance. (It's surprisingly cheap, e.g. Delta Dental offers plans for under $100/yr; lots of people don't make use of their plan and subsidize the treatment of those who do use theirs). Losing teeth greatly increases your chances of infections over time.
Things that will kill you right now
Avoidable medical errors
Avoidable medical errors might be the second leading cause of death after CVD.[1] This makes a hospital visit possibly the most dangerous thing you can do, especially if you are young. In general, you should not assume that medical staff are competent. Triple check dangerous prescriptions. If you don’t know whether a prescription is dangerous, assume it is. Ask medical staff if they’ve washed their hands (yes, this is actually still a major problem). Sharpie on yourself which side of your body a surgery is supposed to happen on, along with your name and what the surgery is for (seriously). Keep your own records, especially if you have serious medical issues; error rates in medical documentation are ridiculous. Medical equipment is generally cleaned by custodial staff with no medical training who often don't know how a particular device works. Have someone you can call in an emergency who knows about all of this.
While we're discussing medicine, I'll throw in a couple low cost recommendations that give me peace of mind, even if an emergency situation is unlikely. The first is that the Red Cross has created an android/iphone app covering first aid with extensive pictures and videos helping you through the situation. The second is quickclot which can stop severe bleeding much faster than traditional techniques.
Unintentional poisoning
This is mostly acetaminophen poisoning resulting from their mandatory inclusion in pain killers to prevent abuse. Also people misdosing themselves with legal and illegal drugs. Be careful, this outweighs traffic accidents in accidental deaths. Adding the 24 hour emergency poison control line number (1-800-222-1222) to your phone is something you can do right now. It is also worth knowing that SOP for acetaminophen poisoning is high dose NAC, which is freely available on amazon in the US (h/t Tara).
Traffic accidents
Michael Curzi has a great post on this I won’t attempt to reproduce here: How to avoid dying in a car crash. It is definitely worth updating your model of what behaviors are dangerous in a car.
Summary of interventions
If you know people who smoke, getting them to vape is the single largest impact you can have on their lifespan.
Pay attention when in your car.
CONSTANT VIGILANCE when dealing with the medical profession and drugs.
Exercise: very high return on first few units of effort, some cardio and some resistance training is best.
Blood donation every 12-24 months for men.
Buy a blood pressure monitor and do blood pressure reduction interventions if needed.
Eat fish, nuts, eggs, fruit, dark chocolate. Supplement Vitamin D3.
Work towards a healthy weight.
If you are losing sleep/are stressed, try one small intervention at a time, and don’t get discouraged. These interventions are the hardest but potentially the most rewarding. Supplements for stress, anxiety, and sleep are somewhat subjective and vary more in reported efficacy than others; self-experimentation is recommended.
Floss (and see a dentist).
Closing
Don’t worry too much. Don’t get down on yourself about health. This creates an ugh field making you less likely to take action. The process of becoming healthier is going to make you feel stupid sometimes. This is a marathon and not a sprint; standard habit forming rules apply. Trying to fix 10 things at once is highly stressful! Do not do this! Discuss things that worked for you and didn’t work for you in the past with yourself and with others and come up with a plan. Don’t publicly commit to your plan in the comments, this makes you less likely to do it. Oh, and feel free to argue with me or request more sources.