5 Answers sorted by
*
140If you wear at least an N95 respirator without a valve, there's no reason to isolate.
Frankly, I find it more than a little annoying that the burden of reducing transmission is not more widely shared with the non-infected. In other words, if high-risk people want to avoid getting covid even after they're fully vaxxed and boosted, they should just wear a respirator rather than relying on the kindness of strangers. Isolation might have made more sense when the PPE supply was limited, but that's no longer the case.
I've found it really hard to find a respirator that seals (judging from the fact my glasses fog), and per microcovid.org that still leaves me with a fair amount of exposure. I imagine many others are in the same boat.
Relying on the kindness of strangers is generally a bad idea, because some strangers are not kind.
(Also, not everyone who is infected knows that they are.)
Maybe I misunderstand your statement. I don't get why you say the burden is on those wanting to avoid rather than those who are infected. Particularly as your first statement is about an infected person taking steps to limit the spread of any residual infection they may still have.
I do have a growing sympathy with the idea that just because you have a case of COVID that necessarily means you need to stay in the leper colony for a while. BUT I'm not sure about where one draws the line on that. Each person's case is a unique so the risk they pose to others needs to be considered on a case by case basis and we still seem to be working that out.
*
60One thing you could do is use microCOVID to look at how risky various events are when the other person has covid, and use that as a baseline to make adjustments off of. For example:
- Outdoors, masked, and ~3 feet away from people for an hour is approximately 150 microcovids.
- Indoors and ~6 feet of distance is about 1,500 microcovids.
- Indoors, ~3 feet of distance and unmasked is about 35,000 microcovids.
From there you can make some educated guesses about how much the risk goes down on day N. Microcovid had a blog post a while ago, pre-delta, that has this image:
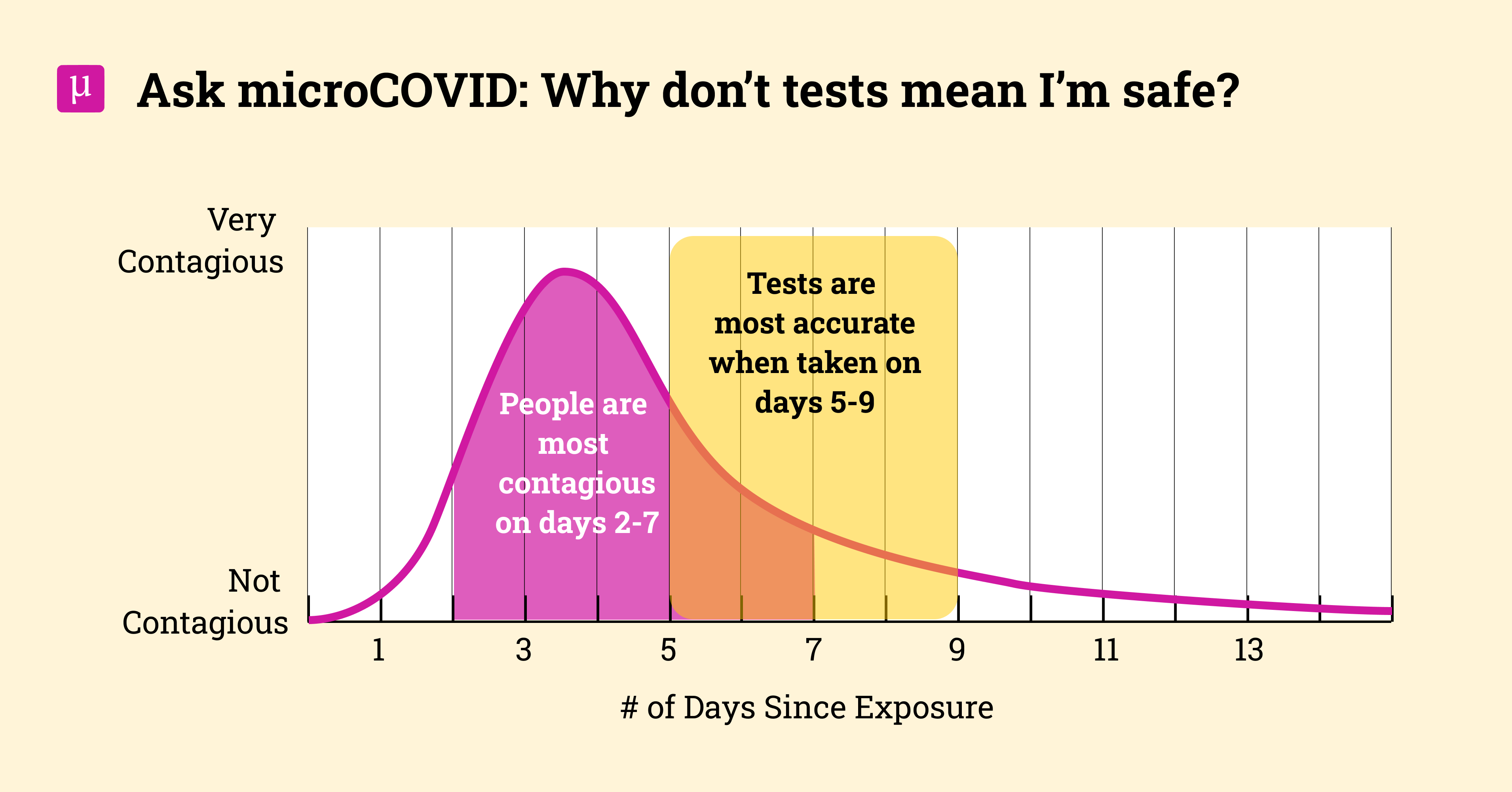
From what I remember about omicron, the infectiousness window is smaller. Ballparking it, I'll throw out some numbers and guess that on day 5 maybe you are 20% as infectious, and on day 10 you are 1% as infectious. Which would yield updated numbers of 30, 300 and 7,000 microcovids respectively for the above scenarious on day 5, and then 1.5, 15 and 350 microcovids for day 10.
So that gives you a sense of how much risk you'd be exposing others to in various situations, which can inform your conclusion on the broader question of how long and in what ways you should isolate for.
40
sniffles don't matter; 10 days after fever's end seems generous/considerate. allegedly positive nasal swab antigen tests will persist for days after it's impossible to lab-culture the virus from a snot sample but in any case such tests are definitely negative after 14 days of onset
Good to know. I wasn't able to take my temperature, but I felt subjectively "feverish" with mild body aches and bizarre dreams on days 1 and 2 and not after. 10 days after that would put me at 12 days of total isolation. If you have any first or second hand sources you can share I'd love to check them out, but I understand if you can't.
30
If you wear a well-fitted n95 (consider sealing the edges to your skin with gentle surgical tape, if you're making do with poorly fitted ones) and keep it on for the entire time, I think any masked activity is acceptable. Then again, wearing a well-fitted n95/KN95/KF94 or better and actually keeping it on is above and beyond what a depressingly high percentage of the population are doing, including most of the healthcare workers I know.
I personally wouldn't consider it appropriate to share air with strangers until after a negative test, but then again, I go out of my way to avoid sharing air with strangers anyways these days and don't find it a major hardship, so I'm probably biased.
I think the major ethical issue of covid these days is making sure not to force anyone to breathe your germs if they don't want to. The argument in favor of doing the CDC-guidelines bare-minimum with respect to restaurants is that, if the restaurant offers a choice between takeaway and indoor seating, everyone who eats indoors is opting into the risk of breathing in what you're breathing out, and not being forced or coerced to be near you in the same way that economic circumstances often force people to shop at grocery stores or ride buses. Those who would rather not breathe strangers' germs, such as myself, get our food to go and eat at home, in a park, or anywhere else we can make ourselves comfortable with good airflow.
I totally agree that ideally I would test negative before sharing air with anyone, especially those who didn't "opt-in" to the risk. Unfortunately antigen likely won't be available in my area, and PCR seems to not be a great indicator of current viral load, so I'm left estimating based on my symptoms/days of isolation. Continuing to isolate is a significant inconvenience/quality of life downgrade for me, but I am able to do it indefinitely without impacting my basic survival needs.
20
This says that 16% of people remain infections at day 7 and 5% of people remain infectious at day 10:
https://ukhsa.blog.gov.uk/2022/01/01/using-lateral-flow-tests-to-reduce-the-self-isolation-period/
Since (1) presumably that study includes people both with and without symptoms at those times (they don’t elaborate on methodology, so I assume they took everyone) and (2) being symptomatic makes you much much more infectious, I would therefore take those numbers as rather serious overestimates.
Case was relatively mild, and I'm feeling a lot better now (day 5), though I still have the sniffles and minor fatigue. I tested negative last week and positive this week via PCR, so I'm pretty confident this was COVID and not an unrelated illness. I live in the US, where CDC guidelines now say I can go into public spaces if my symptoms are "resolving" and I wear a mask, though this feels a little permissive given the requirements of other countries. It's unlikely I will be able to get an antigen test result back before day 10. I'm fully vaccinated and boosted with pfizer as of ~3 months ago. I'm having trouble finding high quality research on infectiousness over time. What do you think is a reasonable amount of time to wait (possibly conditional on symptoms) to do the following? None are essential to my basic needs. I will probably do the median of what the community recommends if it seems well supported.