Here's some information about some of the diseases you have mentioned and their associated vaccines.
Hep A is not routinely offered in the UK because it's considered very low risk there. Even in the US, hep A is usually only something that gets introduced after someone visits a high incidence country. Likely, hep A's risk in the US is partly because we share a border with a high incidence country. Hep A is spread through contaminated food and water, and it takes an incredibly low amount of virus to cause disease in a person. When you get it as an adult, it can lead to some really serious liver complications, and many cases end up hospitalized. Likely, hep A in the UK is because they don't expect to get an influx of people coming in who are infected with hep A. By the way, currently, we are experiencing a hepatitis A outbreak of unprecendented scale and duration in San Diego, CA, and Michigan.
The point of the chickenpox vaccine is only partly to protect the kids. The vaccine will also mean that kids who are vaccinated against chickenpox won't get shingles. Also, when you get it as an adult, it is Bad Times.
Meningococcus vaccine isn't recommended until you're 12 years old. The CBA on it has been a bit back and forth, but this one is likely due to cultural things - meningococcus meningitis outbreaks are common when kids from all sorts of different places end up in one place (aka, college, frats (especially!!), team sports, spending a lot of time in close contact with others). Because the course of the disease is real quick (healthy to dead in less than 24 hours) and morbidity is so bad, it's pretty much recommended due to an abundance of caution. Two years ago, Santa Clara University had a case, and the state responded by mass vaccinating everyone on campus - something like 5,000 people in two days. Such an effort was hideously expensive, but still worth it to the state in terms of morbidity avoided.
Hep B is recommended because 1) there's no cure for it, and 2) having HBV increases your risk of liver cancer by an insane degree. Infection as a kid usually leads to lifetime infection in a carrier state (or to disease progression), whereas infection as an adult is less likely to lead to chronic illness. It's really common in East Asians and Africans, and HBV is also considered endemic in Latin American countries. Of your listed countries, the USA is also the most ethnically diverse. Basically, you're risking putting your kid at risk for liver cancer down the line. Also, HBV costs Medicare a shit ton of money every year in liver transplant/ liver cancer treatment costs.
As a reader of this site, I feel like you should understand that humans are very bad at evaluating small percentages. Under this lens, look at the risk of harm that the vaccination poses to your child, then look at the risk of harm that getting the disease may pose to your child.
The cost benefit analysis you should be doing is how much it will cost you to do this today versus how much pain it's going to cause your kid in the future.
I appreciate your reply.
The government also makes cars have seatbelts and airbags; is this because seatbelt and airbag manufacturers lobbied the government? How dare they make you pay for features you don't want! If you think you're never going to need that airbag, why should you pay for it?
I was going to knee-jerk reply to this and say I'll gladly pay for that because all advanced nations agree that seatbelts and airbags should be standard, but I thought I'd look it up first. Apparently air bags aren't required by the European Commission!
https://ec.europa.eu/transport/road_safety/specialist/knowledge/vehicle/safety_design_needs/cars_en
Thanks for opening my eyes to the air bag conspiracy!!!!1
As a reader of this site, I feel like you should understand that humans are ery bad at evaluating small percentages. Under this lens, look at the risk of harm that the vaccination poses to your child, then look at the risk of harm that getting the disease may pose to your child.
As a reader of this site I expect you would pick up on the fact that I was outsourcing this to national health care systems because humans are bad at researching literature on a scientific field of study without coming to conclusions that support their preconceived notions. Even when they know they're susceptible to this kind of bias.
Thanks for opening my eyes to the air bag conspiracy!!!!1
Haha, right? I definitely did a double take when I first learned that.
As a reader of this site I expect you would pick up on the fact that I was outsourcing this to national health care systems because humans are bad at researching literature on a scientific field of study without coming to conclusions that support their preconceived notions. Even when they know they're susceptible to this kind of bias.
But you're outsourcing without having had asked the right question or acknowledging the subtlety in your outputs.
Your question in particular isn't "what are the only vaccines I should get", it is "how do I best protect the health of my child". If you wanted to ask "which vaccines are absolutely, without a question important to the human race?", then your approach arguably has validity.
I reject the assertion that you are truly outsourcing this to national healthcare systems in good faith, because you admitted to having "fear that a doctor is about to stick my kid with a needle because there was a meeting in a shady room between a pharma rep and a CDC official". Do you have any evidence that that kind of "pharma collusion" isn't happening in any other countries? If you can't believe what some of the experts say because of an unbased/unquantified fear, then what value does any of the evidence have to you at all? If you put arbitrary weights on certain pieces of evidence, then you're weighting it in favor of coming to a conclusion that supports your preconceived notions.
If you're truly outsourcing this information to national health agencies, you would come up with a vaccine list that is the union and not the intersection. After all, they are experts who should know best, so we should defer to them, right? The intersection is merely the list that is your absolute top priority, and the union is the list of vaccines that experts believe are also important.
Like many of the other people in this thread have stated, there's a difference in disease risk and incidence based on where you are living. If you were outsourcing this to national health agencies in order to answer the question of "what do I get to protect the health of my child", then you would weight more highly the guidances of the agencies that are most relevant to you. Instead, you're looking at countries with population sizes that are like, 2% of that of the country you're living in, located in a entirely different geography, with different population dynamics and concentrations, and trying to say that they are 'equal'.
More on the point of looking at the importance of prevalence when making vaccination decisions:
One of the things about infectious diseases is that the more you have of it in a population, the more you tend to get. If prevalence of a disease is really low, even without vaccination, you're not likely to get this disease. This has huge impacts on why some places would recommend it and some other places wouldn't. For example, Denmark doesn't recommend hep B vaccine, but most of the EU does, and so does the US. Denmark's hep B virus prevalence is 0.03%, the EU as a whole guesses around 1%, and the US is at 0.4% (though this number is believed to be an underestimate). You're over 10 times less likely to get hep B if you're living in Denmark vs living in the rest of the EU or the US. Given this information, would you choose to believe Denmark's guideline's or the US' guidelines when making a decision about your US-born child?
I think this post underrates two general rationalist skills, plus some assorted empirical facts. First, the two skills.
Avoiding the fallacy of the one-sided wager. The post talks about cost-benefit analysis, but in a complete cost-benefit analysis one has to consider the risks of both choices under offer, not just one. The post takes specific notice of the default course of action's risks (money, tears, side effects) but focuses less on the risks of the alternative (e.g. toddlers winding up in the ER because they're shitting themselves half to death from rotavirus).
Trying to look things up. I'll pick this point up briefly below.
The rest of this comment is going to be scattershot, as it just runs through relevant facts I was inspired to check or dig up by different bits of the post.
I grew up in the US in the 80s and I don't remember getting nearly this many. Is my memory faulty?
Probably not, there's a simpler alternative explanation: adults remember basically nothing from before age 3 or so. However, we don't even need that explanation, because...
I'm pretty sure it was more like 12 back in those days.
...the CDC actually did recommend fewer vaccines in the 1980s (via). Though this wouldn't address whatever local or state-level vaccine program you might've also experienced as a kid.
Is this all really necessary? Nobody likes getting shots, especially not children. What changed, anyway?
Scientists and clinicians developed and tested newer vaccines and better vaccines. Seriously! (I think this is an example of how people, even very educated people, tend to not understand on a gut level how much of microbiology's progress was made just in the past 40 years.)
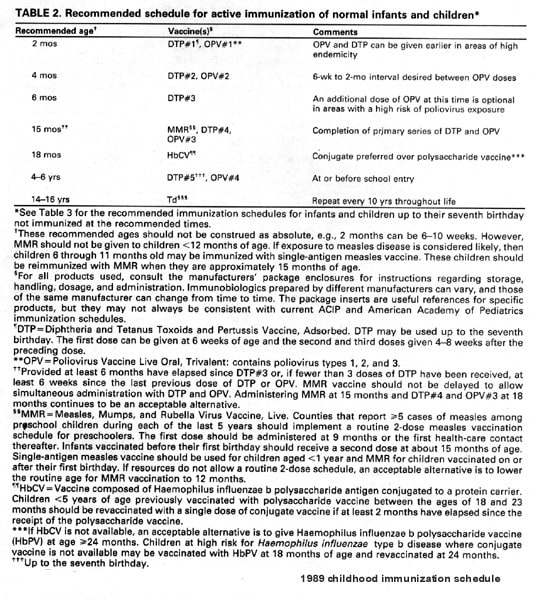
The CDC's 1989 vaccination schedule and current schedule for normal children have only 3 vaccines in common: DTP/DTaP, HbCV/Hib, and MMR. That leaves 7 vaccines which appear on the current schedule but not the 1989 schedule. I looked each of the 7 up online and discovered the following.
A patent on hepatitis B vaccine was filed in 1969, but the earliest actual vaccine appears to have come only in the 1970s. It was shown effective in 1980 and made available in 1981, but the vaccine wasn't ideal for mass vaccination because it came directly from carriers' purified blood and was hard to mass produce. A superior recombinant vaccine came along only in 1986, the first of its kind for humans.
Rotavirus vaccines didn't even get to the point of testing until the 1980s, and the first publicly introduced vaccine arrived only in 1998. And was then promptly withdrawn due to concern over a potential side effect — clinicians & manufacturers do keep an eye open for side effects!
Pneumococcal vaccines have been tested in people for about a century but were relatively ineffective and poorly understood, and their popularity waned with the rise of penicillin. Modern tests began again in 1968 and continued into the 1970s, resulting in US approval for a new vaccine in 1977. However, that vaccine covered only 14 variants of pneumococcus; an improved 23-variant version "covering about 87% of bacteremic pnemuococcal disease in the US" came out in 1983 and was recommended for routine vaccination only in 1984 (and then just in old adults).
Inactivated poliovirus wasn't new (Salk famously developed it in the 1950s) but in the current CDC schedule it merely replaces the oral polio vaccine (OPV) used in the 1980s. The inactivated poliovirus vaccine is safer than the OPV in that children who receive the OPV can crap the live, active virus back out.
Influenza vaccines are even older, dating to the 1930s.
The first varicella vaccine was developed in Japan in the early 1970s, but its safety and worthiness were controversial. Clinical trials took place in the 1980s and the vaccine was licensed for use in Japan in 1986. The US followed suit in 1995.
Hepatitis A vaccine went on the market in the early 1990s. Based on playing with Google Scholar, I think the key human studies were done in the late 1980s and early 1990s.
So we have a mundane explanation for most of the newly introduced vaccines for healthy young children; today's vaccines weren't ready before the '80s.
Now, I'm not an expert on immunology or epidemiology so I expect diving into the literature isn't going to be fruitful; I won't be able to ante up decades of education and experience fast enough.
Don't do yourself down! A lot of material written by clinicians & researchers is out there, some of it deliberately targeted to laypeople, and you can often get some understanding even of technical material just by reading, recalling high-school biology, doing arithmetic, and looking things up in medical dictionaries. You won't learn everything, but if the topic is important to you you can discover a lot by spending a few weekends with Google. (There are topics it's hard to get a hold on as a layperson, but it's hard to know whether a topic's that difficult without trying to get a hold on it.)
Here's how many shots each nation's health care system recommends by the time children turn 5.
37 US
25 UK
I thought I'd take a closer look at these two countries (they're both Anglophone, easiest to check). I get somewhat different numbers: 32 or 33 for the US/CDC (count the yellow boxes, remembering to count the annual flu virus 5 times) and 19 for the UK/NHS (only 4 anti-flu injections here; we don't start them until age 2).
Also, while there's a clear UK-US difference in the number of injections, it's exaggerated by the UK lumping multiple vaccines together into one injection. The UK bundles the DTP, polio vaccine, Hib and hepatitis B vaccines; if I broke those out separately I'd get 29 injections instead of just 19 (and then I'd get 30 if I split the combined Hib/MenC vaccine). The numbers of distinct exposures to microbes are similar in the two countries.
When it comes to cultural and environment differences I have a hard time imagining that the orthodoxy varies because Hep A is a much bigger deal in the US. I presume the calculus changes based on your geographic neighbors, but is it a meaningful difference?
Probably the prevalence of hepatitis A in the US itself plays a bigger role. Trying to summarize hepatitis A's prevalence in different countries is a bit of a pain, because prevalence varies a lot by age and cohort as well as place, but I did find a couple of kinda representative studies of the prevalence of hep. A antibodies in the US and UK. Immediately before (1988-1994) vaccine licensing a national survey found a prevalence of 32% in the US, while a nationwide UK study got a prevalence of 12% in unvaccinated individuals around 2002.
On the flip side of this argument: so what if we vaccinate kids against more diseases than other countries? Well, they're not free. [...] Those other nations (presumably) ran cost-benefit analyses too and came to different conclusions. It would be nice if each country showed their work.
At least 3 of the 5 countries you discuss have shown work. See the US's CDC, the UK's Joint Committee on Vaccination and Immunisation, and Germany's Standing Vaccination Committee at its Robert Koch Institute. Granted, I couldn't find any dedicated webpages for Denmark or Sweden in a few minutes of searching, but that may be due to my non-knowledge of Danish & Swedish.
I haven't digested your entire reply yet, but I'll respond to this part.
- Avoiding the fallacy of the one-sided wager. The post talks about cost-benefit analysis, but in a complete cost-benefit analysis one has to consider the risks of both choices under offer, not just one. The post takes specific notice of the default course of action's risks (money, tears, side effects) but focuses less on the risks of the alternative (e.g. toddlers winding up in the ER because they're shitting themselves half to death from rotavirus).
[...]
So we have a mundane explanation for most of the newly introduced vaccines for healthy young children; today's vaccines weren't ready before the '80s.
The unstated (but I thought implied, my mistake) other-side of the wager was: I got many fewer vaccines growing up, and I'm fine.
Less anecdotally, I haven't found a lot of evidence that adults are suffering horribly from diseases that children today are routinely vaccinated against. Is the cost-benefit of the added vaccines as good as the cost-benefit of the 80s era vaccines? Some arrows point to the US having a lower threshold for recommending them, given the variance between nations.
Less anecdotally, I haven't found a lot of evidence that adults are suffering horribly from diseases that children today are routinely vaccinated against. Is the cost-benefit of the added vaccines as good as the cost-benefit of the 80s era vaccines? Some arrows point to the US having a lower threshold for recommending them, given the variance between nations.
A lot of the big childhood vaccines are things that kill kids (MMR, rotavirus, Hib). So you've got survivorship bias there.
As for the other stuff, a lot of the diseases that adults are suffering from that children are vaccinated against today don't manifest as obvious infectious disease. If you know anyone who has ever had shingles, you know someone that had suffered from a disease that children today are routinely vaccinated against (varicella). If you know someone who has had cervical cancer or genital warts, you likely know someone who has suffered from HPV (highly recommended vaccine for preteens). If you know someone who has had liver cancer, there's a chance it's because of Hepatitis B (no vaccine for HCV yet :/).
Of course, you don't have to look anecdotally for that.
Part of the cost benefit change is also due to the fact that we can actually treat a lot of these cancers now, instead of just "sorry, nothing we can do, go home and get your affairs in order." For example, even though mortality rates from liver cancer might still be similar, 1-year survival rates have increased. So now, each case of a preventable cancer might cost us a lot more, so we're much more motivated to prevent it.
Even if the cost benefit is not as good as the cost benefit of the 80s era vaccines, the fact that many not only have a favorable cost-benefit ratio, but are even cost saving should make them an strong choice for implementation.
It seems like you're trying to analyze the wrong things. Second-guessing motives for recommendations that apply to large variant populations is a losing game, and you missed what may be a fairly large reason: prevalence of the disease in that region. In any case, ignore politics and look at expected value and risks of each option AS IT APPLIES TO YOU.
Where will you be living/visiting? What is the actual incidence and cost of these diseases, and what are the network effects of many people being immunized vs not? I worry that you think the biggest cost of chicken pox is staying home with a sick kid - the actual biggest risk is that the kid WON'T get it as a kid (because all the neighbors and other kids are immunized), and will instead get it as an adult when it can be very serious.
Shots aren't terribly expensive, the pain of the stick is fleeting, and the chance of serious side-effects is quite low. Compare that to the pain and probability of the disease, and I'd generally say take all you can get. My default would be the union of recommendations for anywhere I expect the kid to visit, rather than the intersection.
"When it comes to needles to stick my new kiddo with, I'm not really being persuaded to do more than the intersection of vaccinations between similar nations."
You don't know enough to decide this. What is "similar" (climate, culture, disease spectrum?) Do you know the history of their immunization laws?
Seems to me you first decided this is an icky procedure, and it hurts your kid, and you feel protective. Then you went looking for reasons not to do it. Immunization has a free-rider aspect, because of herd immunity. So you may well get away with it, in terms of your kid's health, but "people like you" (defectors in PD) are a problem.
If you are an evil pharma-corp, vaccines are a terrible way to be evil.
C/D calculations in public health are real, but this is one of those things where the only way to be effective is not break the phalanx formation.
When it comes to needles to stick my new kiddo with, I'm not really being persuaded to do more than the intersection of vaccinations between similar nations."
You don't know enough to decide this. What is "similar" (climate, culture, disease spectrum?) Do you know the history of their immunization laws?
That's incorrect. I know that my generation was vaccinated against a more limited set of diseases and has survived pretty well.
It's not wrong to question US health orthodoxy when it's not at all a secret that pharma can influence US policy and other similar nations haven't followed these recommendations.
Seems to me you opened a bottle of righteous indignation for me that you had saved up for someone else..
That's incorrect. I know that my generation was vaccinated against a more limited set of diseases and has survived pretty well.
"There's no need for the smartphones. I know that my generation only had landlines to use, and has survived pretty well."
"Back in the day, smallpox was just a fact of life. Most people lived. What's the big deal about it anyway, afterall, we survived pretty well, and it's not like it was holding our society back"
"Why do we need to wash our hands before surgery? We've survived pretty well so far like this."
Just because you have not personally seen someone die from a vaccine preventable disease doesn't mean that it doesn't happen, or that it's okay.
http://callingbullshit.org/videos.html
(a) You don't know enough to decide one way or the other.
(b) If (a) is true, trust your local public health person.
If you are an evil pharma-corp, vaccines are a terrible way to be evil.
Evil pharma-corps don't care about being evil but care about making money. I don't see why vaccine that can be sold Westerns are bad on that front.
Depends on what else is in EvilPharmaCorp's portfolio. Vaccines are generally cheap, but broadly applied so can be profitable. Treatments for disease are often CRAZY expensive, but you sell less of them. There is a network relationship, though - if you can sell much less of the vaccine, you can increase the disease more than linearly.
So truly evil pharma would try to suppress immunization rather than pushing it.
There are enough different pharma companies that vigorously compete with each other. One company that has a patented treatment for disease X that makes a lot of money might not want to develop a vaccine to cure it but that doesn't mean that developing a vaccine isn't interesting for other companies.
I agree with most of what you've said, but here's a quibble:
If you are an evil pharma-corp, vaccines are a terrible way to be evil.
Unless you're one of the sellers of vaccines, right?
Is this all really necessary?
Necessary is a bad word. The core question is what happens to be the highest utility.
In the US we also recommend: Hep A, Hep B, Rotavirus, Meningococcus, Varicella, and yearly flu shots (for babies and children).
Meningococcus, Rotavirus and Varicella also seems to be on the schedule in Germany. The first three I Googled.
It would be nice if each country showed their work.
Every country does has a commission that argues their decisions. From your perspective the problem is likely that the German documents are in German, the Danish in Danish and the Swedish in Swedish.
{kind=link}
I'm about to have a baby. Any minute now. Well, my partner is. I'm just sitting here not growing a baby wondering what to do with myself.
Maybe I can get a jump on our approach to medical care for the new kiddo.
One thing that sticks out at me is that children in the US get a lot of vaccinations. At my quick count it's something like 37 shots by the time they're 5.
I grew up in the US in the 80s and I don't remember getting nearly this many. Is my memory faulty? I'm pretty sure it was more like 12 back in those days. Is this all really necessary? Nobody likes getting shots, especially not children. What changed, anyway?
Now, I'm not an expert on immunology or epidemiology so I expect diving into the literature isn't going to be fruitful; I won't be able to ante up decades of education and experience fast enough. Presumably this is what we pay people at the US CDC and Department of Health for.
But can you *really* trust them? Aren't all of these vaccinations really convenient for the pharmaceutical industry? Aren't there seemingly constant allegations/lawsuits about the over-prescription of drug interventions in the US?
The health care systems in major world countries have access to all of the same literature, and they're presumably staffed by educated, expert people too so they should all come to the same conclusions as the US system right? Not so!
Here's how many shots each nation's health care system recommends by the time children turn 5.
37 US
25 UK
25 Germany
16 Sweden
16 Denmark
The intersection of vaccines being recommended are TDAP, MMR, Polio, HIB and PCB.
In the US we also recommend: Hep A, Hep B, Rotavirus, Meningococcus, Varicella, and yearly flu shots (for babies and children).
Can we explain the variance? I can think of a few reasons they would vary.
1. Cultural bias. This can be big. A psychiatrist in the UK told me that they're not as pharma heavy as, say, psychiatrists in Germany because of a WW2 era bias: lots of the big pharma companies are German.
2. Cultural and environmental differences. Some diseases are a bigger deal in some countries than others. Japan (not included above) recommends immunization against diseases (TB, Japanese encephalitis) that none of the systems above are too concerned with.
3. Undue industry influence. Run-of-the-mill corruption.
4. Quality of health care systems and social safety nets vary.
When it comes to cultural and environment differences I have a hard time imagining that the orthodoxy varies because Hep A is a much bigger deal in the US. I presume the calculus changes based on your geographic neighbors, but is it a meaningful difference? Or is it a counterproductive cultural bias? For example, in the US we may spend more time thinking about diseases people in central America suffer from than the people in Denmark might, but do the neighbors in this case meaningfully translate to a higher disease risk? Or are we vaccinating against unfounded fears?
Do the other nations vaccinate less than the US because their health care systems are worse? Annoyingly (if you're an American) all of their health care outcomes rank better.
Is the US health care system more corruptible by industry influence?
Is the story a lot simpler and less sinister? That the US vaccinates more than the rest of these countries because the balance of the US's health care system (access to treatment, quality of treatment) is worse? Or is it because having to stay home with a kid that's sick with chicken pox (varicella) is not so big a deal in, say, Denmark, because the social contract is more forgiving of parents who miss work?
Does the poorer quality of health care in the US (going by international rankings) and the lower tolerance for parents missing work combine poorly with the undue influence of industry and therefore lead to more vaccinations?
On the flip side of this argument: so what if we vaccinate kids against more diseases than other countries? Well, they're not free. They cost money to administer, and cost tears because kids hate getting shots. The health risks from vaccines aren't zero, either. Vaccines have side-effects, and sometimes they're serious. Those other nations (presumably) ran cost-benefit analyses too and came to different conclusions. It would be nice if each country showed their work.
When it comes to needles to stick my new kiddo with, I'm not really being persuaded to do more than the intersection of vaccinations between similar nations. The fear that a doctor is about to stick my kid with a needle because there was a meeting in a shady room between a pharma rep and a CDC official is pretty powerful. It doesn't seem like a strictly irrational concern either