Conscious Proprioception.
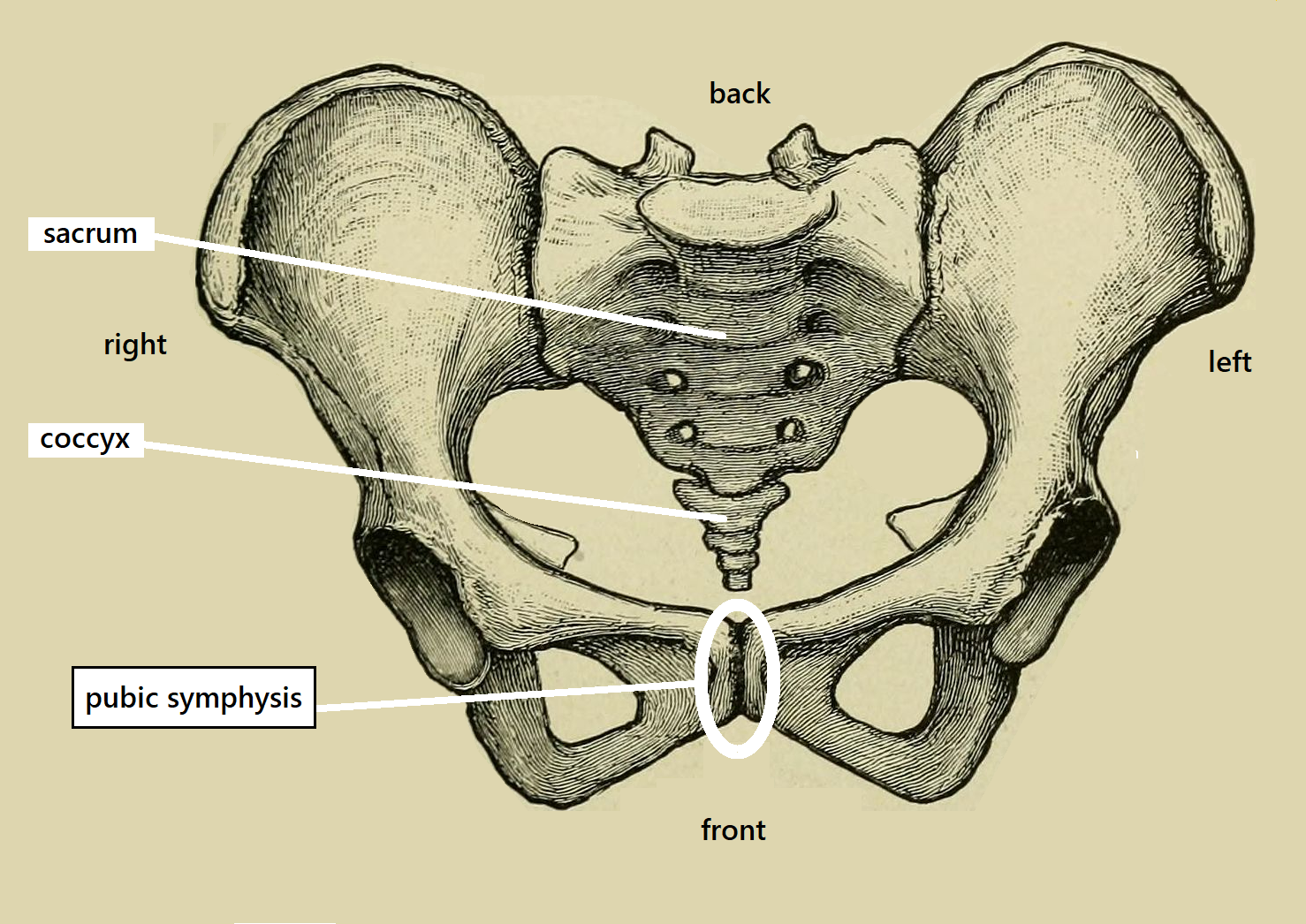
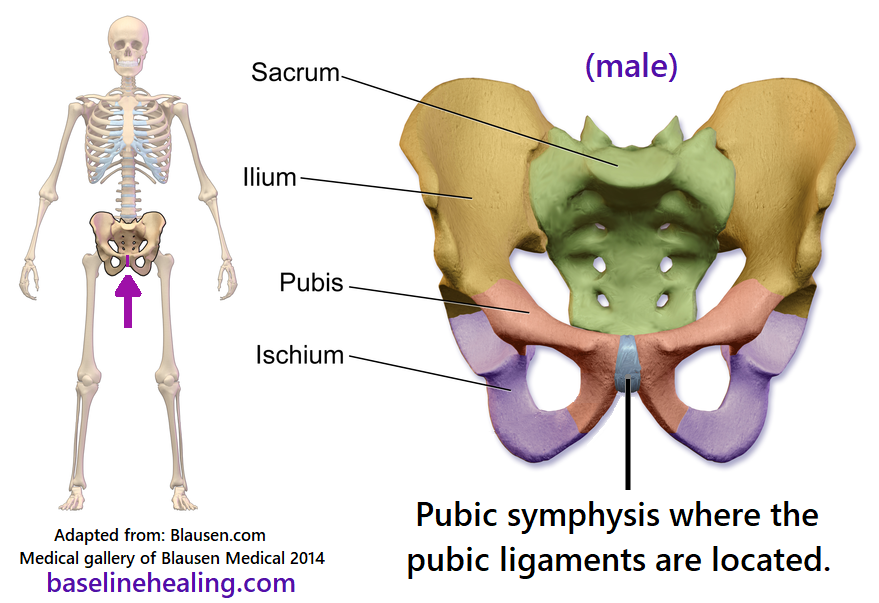
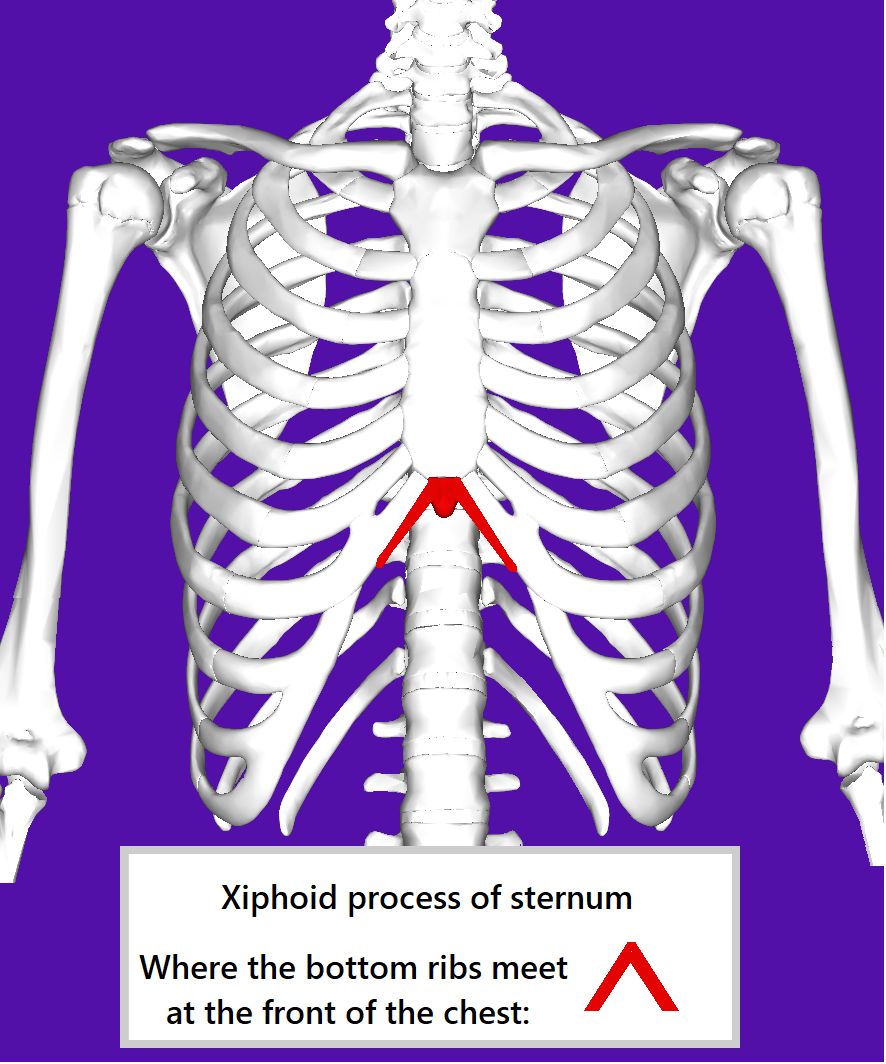
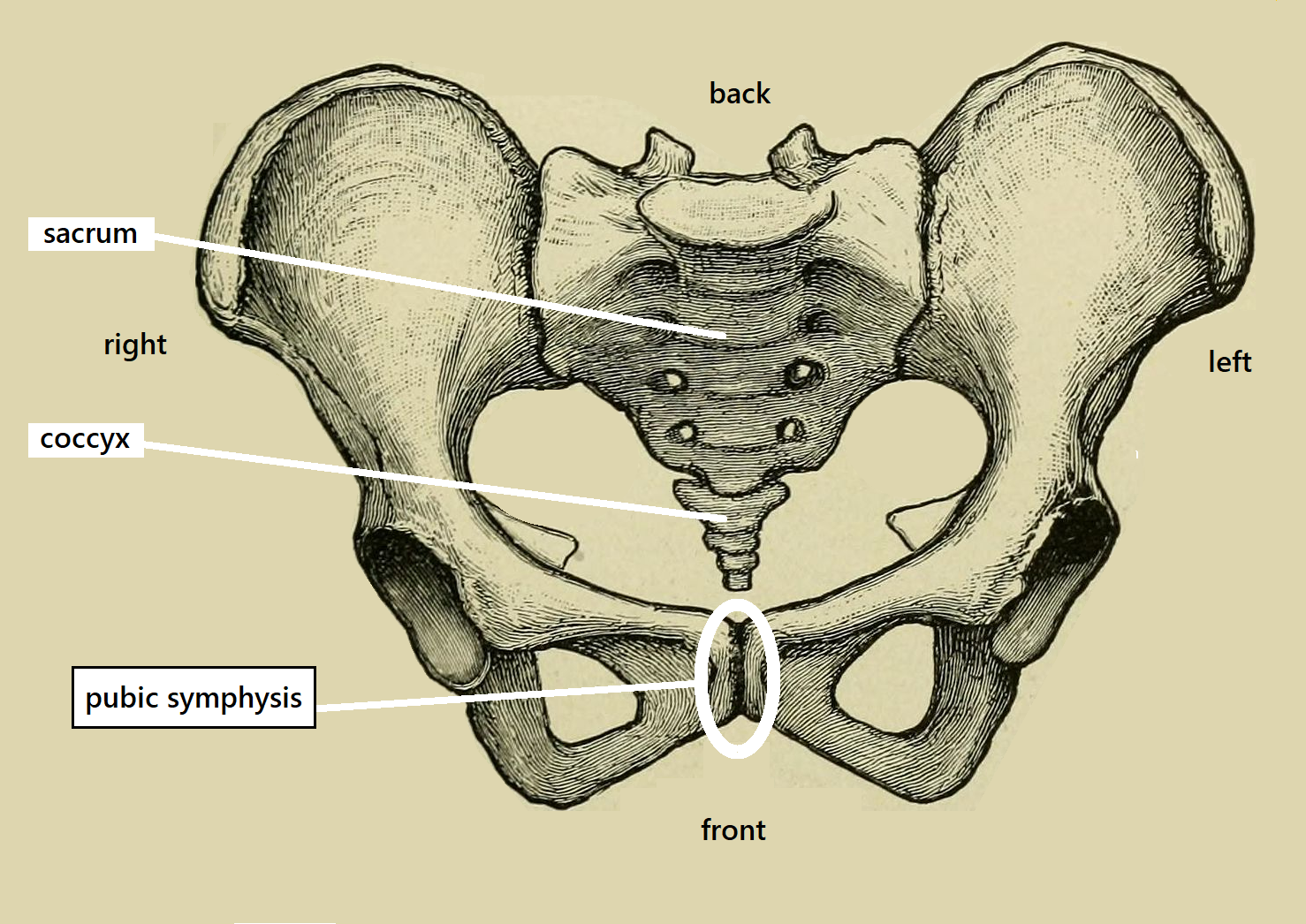
Conscious Proprioception: Increased Awareness of your Sense of Position, Motion, Alignment & Balance. After an introduction to the anatomy of alignment and balance and the 5 main muscles of movement, consider what you experience if you focus on the position (posture) and motion of your body: How much of your sense of proprioception are you aware of ? Origin page is located here: conscious proprioception @ baselinehealing.com Introduction. Standard definition of proprioception: > Proprioception: "The ability to sense stimuli arising within the body regarding position, motion, and equilibrium." The basic physiological model of proprioception: * 'Sensors' located throughout the body generate sensory feedback, 'information' that is sent, via the nervous system, to the brain. Sensory feedback concerning the body's position, motion and balance is our sense of proprioception. * The brain 'processes/interprets' this feedback about positioning and then sends signals around the body to maintain a 'functional posture', the positioning of the body that we use day-to-day. I feel it fair to say that the different mechanisms and various proprioceptors ('sensors') involved in proprioception are far from being understood and our sense of "bodily awareness" appears in the philosophical section at Stanford. This post is my attempt to explain my experience of an increased consciousness of the proprioceptive feedback my body is continually producing - and how everyone can increase their awareness of their physical selves - feeling the positioning of the parts of your body, your state of motion and equilibrium. Conscious proprioception. Awareness of: * The relative position of the parts of your body. * The motion of your body. * Your equilibrium - whether you are balanced or not. According to: Base-Line Theory of Health and Movement. (part 2) (BLTH part 1) Increased awareness of the body's positioning, balance and state of alignment - of the body's posture - com






{kind=link}
A new paper that might be of interest:
Recalibrating SARS-CoV-2 Antigen Rapid Lateral Flow Test Relative Sensitivity from Validation Studies to Absolute Sensitivity for Indicating Individuals Shedding Transmissible Virus