If you are keeping schools open in light of the graphs above, and think you are not giving up, I don’t even know how to respond.
I think the French lockdown probably won't work without school closures, and this probably will be noticed soon when the data comes through establishing that it doesn't work, and I think that it's extremely dumb to not close schools given that the risk for closing vs not closing at this point is extremely asymmetric, but this isn't 'giving up' knowingly (and I infer that you're suggesting Macron may be trying to show that he is trying while actually giving up) - this is simply Macron and his cabinet not intuitively understanding asymmetric risk and not realizing that it's much better to do far more than what was sufficient, compared to doing something that just stands an okay chance of being sufficient to suppress, in order to avoid costs later.
I think that there is a current tendency - and I see it in some of your statements about the beliefs of the 'doom patrol' - to use signalling explanations almost everywhere, and sometimes that shades into accepting a lower burden of proof, even if the explanation doesn't quite fit. For example, the European experience over the summer is mostly a story of a hideous but predictable failure to understand the asymmetric risk and costs of opening up / investing more vs less in tracing, testing and enforcement.
Signalling plays a role in explaining this irrationality, certainly, but as I explained in last week's comment wedging everything into a box of 'signalling explanations' doesn't always work. Maybe it makes more sense in the US, where the coronavirus response has been much more politicised. Stefan Schubert has a great blog post on this tendency:
It seems to me that it’s pretty common that signalling explanations are unsatisfactory. They’re often logically complex, and it’s tricky to identify exactly what evidence is needed to demonstrate them.
And yet even unsatisfactory signalling explanations are often popular, especially with a certain crowd. It feels like you’re removing the scales from our eyes; like you’re letting us see our true selves, warts and all. And I worry that this feels a bit too good to some: that they forget about checking the details of how the signalling explanations are supposed to work. Thus they devise just-so stories, or fall for them.
This sort of signalling paradigm also has an in-built self-defence, in that critics are suspected of hypocrisy or naïveté. They lack the intellectual honesty that you need to see the world for what it really is, the thinking goes
I think that a few of your explanations fall into this category.
They’re pushing the line that even after both of you have an effective vaccine you still need to socially distance.
Isn't this... true? Given that an effective vaccine will take time to distribute (best guess 25 million doses by early next spring), that there will be a long period where we're approaching herd immunity and the risk is steadily decreasing as more people become immune, Fauci is probably worried about people risk compensating during this interval, so he's trying to emphasise that a vaccine won't be perfectly protective and might take a while, maybe exaggerating both claims, while not outright lying. I agree that this type of thinking can shade into doom-mongering and sometimes outright lying about how long vaccines might take but this seems like solidly consequentialist lying to promote social distancing (SL 2), not bullshitting (SL 3). Maybe they've gotten the behavioural response wrong, and it's much better go be truthful, clear and give people reasonable hope (I think it is), but that's a difference in strategy, not pure SL3 bullshit. Why are you so confident that it's the latter?
I don’t think this is something being said in order to influence behavior, or even to influence beliefs. That is not the mindset we are dealing with at this point. It’s not about truth. It’s not about consequentialism. We have left not only simulacra level 1 but also simulacra level 2 fully behind. It’s about systems that instinctively and continuously pull in the direction of more fear, more doom, more warnings, because that is what is rewarded and high status and respectable and serious and so on, whereas giving people hope of any kind is the opposite. That’s all this is.
That's a bold claim to make about someone with a history like Fauci's, and since 'the priority with first vaccinations is to prevent symptoms and preventing infection is a bonus' is actually true, if misleading, I don't think it's warranted.
This just sounds exactly like generic public health messaging aimed at getting people to wear masks now by making them not focus on the prospect of a vaccine. Plus it might even be important to know, especially when you consider that vaccination will happen slowly and Fauci doesn't want people to risk compensate after some people around them have been vaccinated but they haven't been. I don't think Fauci is thinking beyond saying whatever he needs to say to drive up mask compliance right now, which is SL 2. Your explanation that Dr Fauci has lost track of whether or not vaccines actually prevent infection might be true - but it strikes me as weird and confusing, something you'd expect of a more visibly disordered person, and the kind of thing you'd need more evidence of than what he said in that little clip. I think those explanations absolutely have their place, especially for explaining some horrible public health messaging by some politicians and public-facing experts and most of the media, but I think this particular example is overuse of signalling explanations in the way argued for in the article I linked above. At the very least I think the SL2 consequentalist lying explanation is simpler and has a plausible story behind it, so I don't know why you'd go for the less clear SL3 explanation with apparent certainty.
Essentially, Europe chose to declare victory and leave home without eradication, and the problem returned, first slowly, now all at once, as it was bound to do without precautions.
We did take plenty of precautions, they were just wholly inadequate relative to the potential damage of a second wave. A lot of this was not understanding the asymmetric risk. Most of Europe had precautions that might work and testing and tracing systems that were catching some of the infected and various shifting rules about social distancing and it was at least unclear if they would be sufficient. I can't speak about other countries, but people in the UK were intellectually extremely nervous about the reopening and most people consistently polled saying it was too soon to reopen. For a while it worked - including in July when there was a brief increase in the UK that was reversed successfully. The number of people I see around me wearing masks has been increasing steadily ever since the start of the pandemic. So it was easy and convenient to say, 'it's a risk worth taking, it's worked out so far' at least for a while - even though any sane calculation of the risks should have said we ought to have invested vastly more than we did in testing, tracing, enforcement, supported isolation etc. even if things looked like they were under control.
Not that giving up is obviously the wrong thing to do! But that does not seem to be Macron’s plan.
...
We are going to lock you down if you misbehave, so if you misbehave all you’re doing is locking yourself down. She’s right, of course, that things will keep getting worse until we change the trajectory and make them start getting better, but no the interventions to regain control are exactly the same either way. You either get R below 1, or you don’t. Except that the more it got out of control first, the more voluntary adjustments you’ll see, and the more people will be immune, so the more out of control it gets the easier it is to control later. ...
And also the longer you wait, the longer you have to spend with stricter measures.
The measures don't need to be stricter unless you can't tolerate as long with high infection rates, in which case you need infection rates to go down much faster. I don't know if makes me and Tyler Cowen and most epidemiologists part of the 'doom patrol' if we say that you'll need a longer interval of either voluntary behaviour change to avoid infection or a longer lockdown the more you wait.
(Note that I'm not denying that there are such doomers. Some of the things you mention, like people explicitly denying coronavirus treatment has made the disease less deadly and left hospitals much better able to cope, aren't really things in Europe or the UK and I was amazed to learn people in the US are claiming things that insane, but we have our own fools demanding pointless sacrifices - witness the recent ban Wales put on buying 'nonessential goods' within supermarkets)
If by 'giving up' you mean 'not changing the government mandated measures currently on offer to be more like a lockdown', given the situation France is in right now, it seems undeniably the wrong thing to do to rely on voluntary behaviour changes and hope that there's no spike that overwhelms hospitals (again, asymmetric risk!) - worse for the economy, lives and certainly for other knock-on effects like hospital overloading. A lot of estimations of the marginal cost of suppression measures completely miss the point that the costs and benefits just don't separate out neatly, as I argue here. Tyler Cowen:
I think back to when I was 12 or 13, and asked to play the Avalon Hill board game Blitzkrieg. Now, as the name might indicate, you win Blitzkrieg by being very aggressive. My first real game was with a guy named Tim Rice, at the Westwood Chess Club, and he just crushed me, literally blitzing me off the board. I had made the mistake of approaching Blitzkrieg like chess, setting up my forces for various future careful maneuvers. I was back on my heels before I knew what had happened.
Due to its potential for exponential growth, Covid-19 is more like Blitzkrieg than it is like chess. You are either winning or losing (badly), and you would prefer to be winning. A good response is about trying to leap over into that winning space, and then staying there. If you find that current prevention is failing a cost-benefit test, that doesn’t mean the answer is less prevention, which might fail a cost-benefit test all the more, due to the power of the non-local virus multiplication properties to shut down your economy and also take lives and instill fear.
You still need to come up with a way of beating Covid back.
'Giving up' is not actually giving up. At least in Europe, given the state of public behaviour and opinion about the virus, 'giving up' just means Sweden's 'voluntary suppression' in practice. There is no outcome where we uniformly line up to variolate ourselves and smoothly approach herd immunity. The people who try to work out the costs and benefits of 'lockdowns' are making a meaningless false comparison between 'normal economy' and 'lockdown:
First and foremost, the declaration does not present the most important point right now, which is to say October 2020: By the middle of next year, and quite possibly sooner, the world will be in a much better position to combat Covid-19. The arrival of some mix of vaccines and therapeutics will improve the situation, so it makes sense to shift cases and infection risks into the future while being somewhat protective now. To allow large numbers of people today to die of Covid, in wealthy countries, is akin to charging the hill and taking casualties two days before the end of World War I.
...
What exactly does the word “allow” mean in this context? Again the passivity is evident, as if humans should just line up in the proper order of virus exposure and submit to nature’s will. How about instead we channel our inner Ayn Rand and stress the role of human agency? Something like: “Herd immunity will come from a combination of exposure to the virus through natural infection and the widespread use of vaccines. Here are some ways to maximize the role of vaccines in that process.”>In that sense, as things stand, there is no “normal” to be found. An attempt to pursue it would most likely lead to panic over the numbers of cases and hospitalizations, and would almost certainly make a second lockdown more likely. There is no ideal of liberty at the end of the tunnel here.
In Europe, we will have more lockdowns. I'm not making the claim that this is what we should do, or that this is what's best for the economy given the dreadful situation we've landed ourselves in, or that's what we'll almost certainly end up doing given political realities - though I think these are all true. What I'm saying is that, whether (almost certainly) by governments caving to political pressure or (if they hold out endlessly like Sweden) by voluntary behaviour change, we'll shut down the economy in an attempt to avoid catching the virus. Anything else is inconceivable and requires lemming-like behaviour from politicians and ordinary people.
So, given that it's going to happen, would you rather it be chaotic and late and uncoordinated, or sharper and earlier and hopefully shorter? If we're talking about government policy, there really isn't all that much compromise on the marginal costs of lockdowns vs the economy to be had if you're currently in the middle of a sufficiently rapid acceleration.
I think that it's extremely dumb to not close schools given that the risk for closing vs not closing at this point is extremely asymmetric
Having a lockdown costs political capital. Having the school continuing to be open means it costs less political capital and there's more room for having the lockdown for a longer period of time. It's not an easy tradeoff.
I think your argument about this line is unfair:
They’re pushing the line that even after both of you have an effective vaccine you still need to socially distance.
Fauci isn't the leader of The Doom Patrol or even, arguably, a member of it. Yes, he might be 'consequentially' lying at SL2 instead of fully bullshitting at SL3, but that seems much less true of the typical members of The Doom Patrol.
You could have also, charitably, interpreted "even after both [?] of you have an effective vaccine" as 'a vaccine is widely available and it's been administered to enough people to create (strongly) effective immunity'. We already have several vaccines that seem to work. And, after you've received the vaccine, it certainly seems reasonable to infer that one's own need to socially distance is significantly less than before.
Your explanation that Dr Fauci has lost track of whether or not vaccines actually prevent infection might be true - but it strikes me as weird and confusing, something you'd expect of a more visibly disordered person, and the kind of thing you'd need more evidence of than what he said in that little clip.
That makes sense given that you seem skeptical of signaling explanations in general. But it also seems like you're arguing that no one operates at SLs beyond 2 without being a "visibly disordered person", which doesn't seem true in general.
My own view is that intelligence and expertise generally make it easier (and thus, all else equal, more likely) for someone to operate at higher SLs. Like rationalization, it often seems like smarter people are much better at this than others; not vice versa.
But again, for Fauci specifically, I agree – in this case – he's probably at SL2. But the rest of The Doom Patrol seems pretty clearly and reasonably at SL3 most of the time.
We did take plenty of precautions, they were just wholly inadequate relative to the potential damage of a second wave. A lot of this was not understanding the asymmetric risk. Most of Europe had precautions that might work and testing and tracing systems that were catching some of the infected and various shifting rules about social distancing and it was at least unclear if they would be sufficient.
I think Zvi's implicitly assuming that 'we' (his readers) mostly know that the precautions were not sufficient. As-of when this post was written, that certainly seems like a reasonable conclusion regardless of anyone's previous thinking.
I don't know if makes me and Tyler Cowen and most epidemiologists part of the 'doom patrol' if we say that you'll need a longer interval of either voluntary behaviour change to avoid infection or a longer lockdown the more you wait.
You don't seem like a member of The Doom Patrol, and Cowen definitely isn't, but I'm ignorant of "most epidemiologists" – you and Cowen are open to discussing SL1, the object level!
I'm not sure why a lockdown would need to be longer "the more you wait". Wouldn't the strictest lockdown only need to last a little longer than the length of the virus's 'infection cycle'?
Assuming that the 'strictest' lockdown isn't possible, which seems reasonable for most places, then I can see the logic of this claim and think it's sensible.
At least in Europe, given the state of public behaviour and opinion about the virus, 'giving up' just means Sweden's 'voluntary suppression' in practice.
This is a good point and the mistake you describe is one I've seen fairly frequently. But I don't think Zvi disagrees.
But, just like a 'government' can give up but not its people, so too can some people give up, but not others. And 'giving up' isn't really a binary decision, for governments or people.
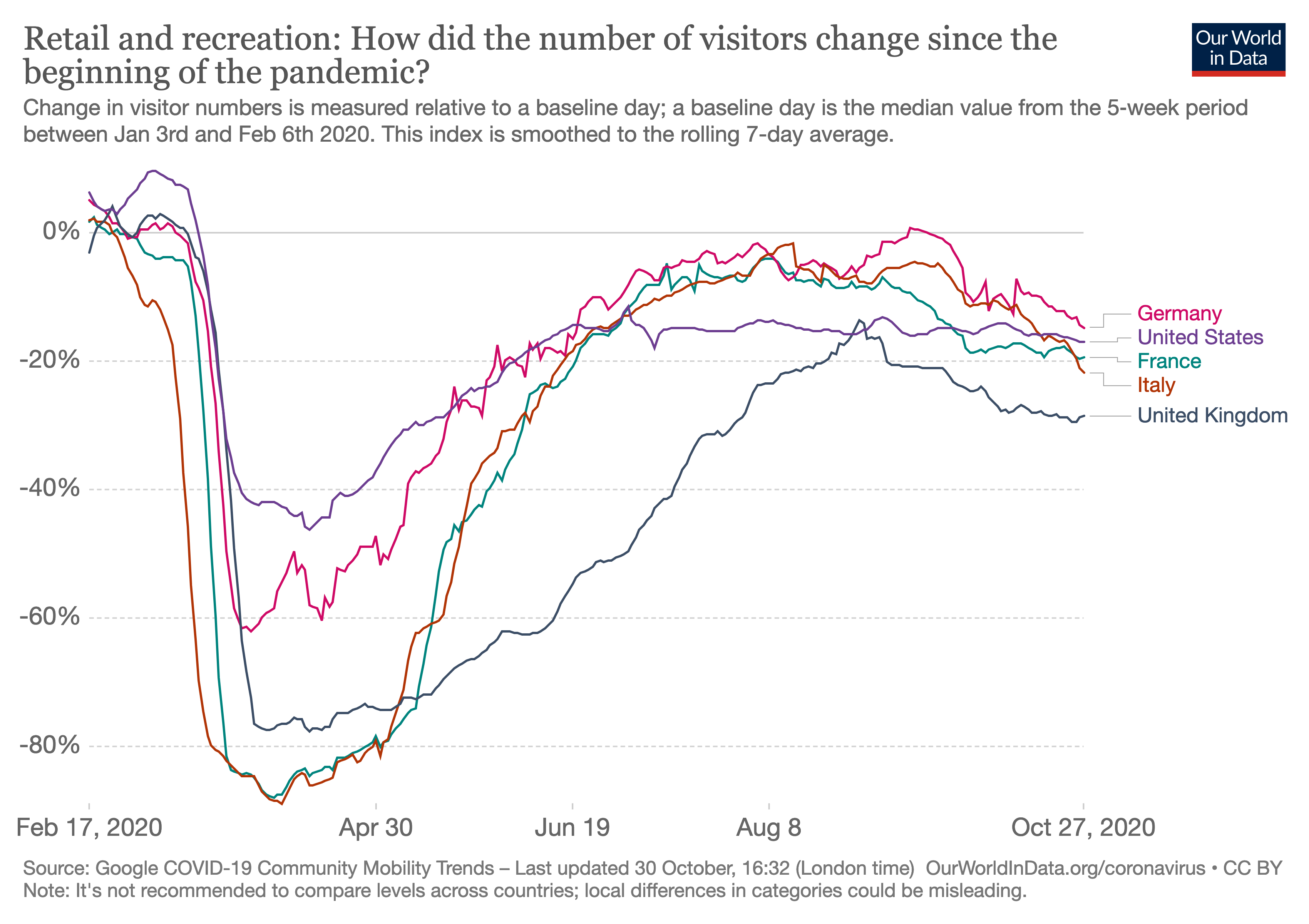
It's not a news source, but I find the Google and Apple Mobility data for Europe to be a useful measure of "how people are actually behaving on the ground". If people are going to retail/recreation locations (rather than ordering online), they are probably not taking the pandemic that seriously. Much of Europe eased up more than US before it had a rapid growth of cases (starting in August/Sep), and behavior hasn't changed much since this rapid growth.
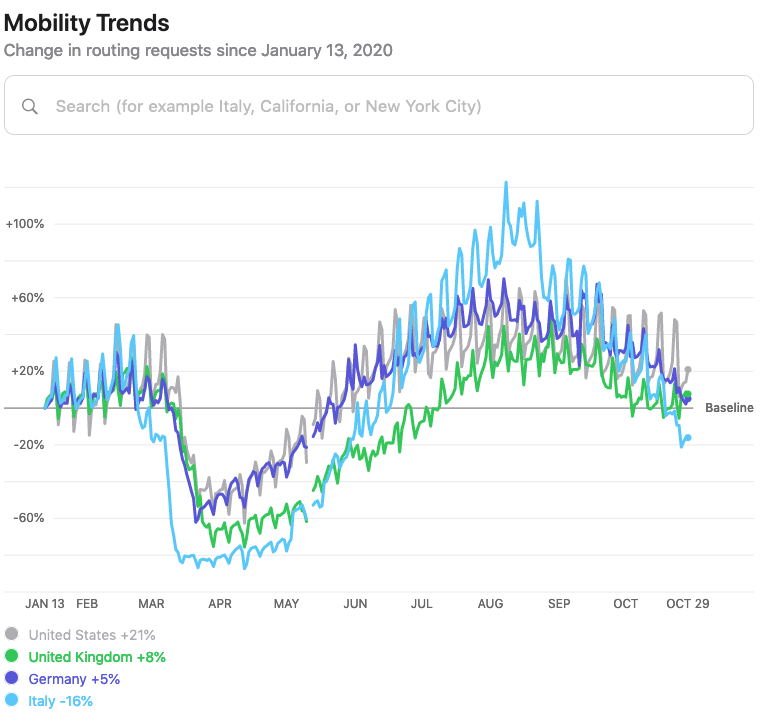
https://covid19.apple.com/mobility
Is there an 'official' way to do this?
If not, and a 'sequence' is 'just' a post linking to a bunch of other posts, it should be easy enough for anyone to make the sequence post.
Maybe the site admins could 'transfer' the post to Zvi afterwards, which would be ideal long-term.
Dr. Fauci quote source turns out to have been misquoting him. The fault is in the journalists this time, not Fauci. I have corrected the original post, please reimport.
The update hasn't made its way here yet, so I'll copy the relevant paragraphs from the updated blog post:
Good news! In an edit to correct a previous version of this post, Dr. Fauci has NOT thrown in with the eternally sacrificing scaremongers, who hereafter will be referred to as the Doom Patrol, by telling us that the vaccines will not block infection. I apologize to him and to all for the error. Instead, it is the headline writers and summarizers who took his true statement – that the vaccines are being tested and measured for preventing illness rather than testing for whether the person is infectious – and transformed that into “Dr. Fauci says early Covid vaccines will prevent symptoms, not block infections.”
That’s what the Doom Patrol does. It takes everything and uses it as a tool to show everything in the worst possible light.
Regarding the question to what extent a vaccine will be able to prevent infection or primarily reduce the symptoms one of Germany's leading virologist, Christian Drosten, made some interesting remarks in his regular podcast this week on public radio (own translation with the help of deepl.com):
"Q: Is there also hope for such vaccines, which actually stop the virus completely, because they can elicit an immune response that is the same as in a real natural infection?
Christian Drosten: With the current vaccines that are currently being tested, this will probably not work. We are dealing here with an infection of the mucous membrane, i.e. in the nose and throat and then later in the lungs - or in the bronchial system, which is more likely to be mucous membrane. And the mucous membranes already have their own special local immune system. With the current vaccines, which are more likely to be administered to the muscles, this local immune system is not as easily reached, i.e. not in the special way. There one has more the general immune effect for the whole body, thus for the systemic spread and also for a part of the general immune response. For example the IGA-antibodies, which then already arrive. IGG antibodies also arrive in the lungs, for example, especially in the context of an incipient inflammation. And this is what the current vaccines do, which probably protect against the severe course of the disease rather than against the infection in general. That's the most important thing we have to do for the time being. There won't be one vaccine for everyone in the beginning anyway. Of course, we have to provide the people at risk with a vaccine and take away the dangerous course of the disease, so that the virus will then lose this high death rate in the population.
Q: If we want to contain the spreading at the same time or at a later stage with vaccines, then one must directly go to the mucous membranes.
Christian Drosten: You definitely have to. One can perhaps imagine it in such a way, the next generation of the vaccines must also contain that.
...
Q: How we get to the mucous membranes.
Christian Drosten: In general this is what we would like to have, vaccines that protect the mucous membranes. That stimulate the special immune system there, so that in the future someone, if he breathes a whole load of virus into the nose, is not infected at all, thus does not get only a mild infection, but no infection at all. The virus is immediately stopped in the nose. And the good news is that some of the vaccines now being tested already contain that. They would even be able to do that already. There is an interesting study that proves this. But in principle, we have known that for quite some time, because these are vector vaccines. In other words, there are always vaccines that are mediated via a viral vector.
Q: Another carrier virus.
Christian Drosten: Exactly, where there is a carrier virus. Only one component of the SARS2 virus is added to this carrier virus, namely the surface protein. These carrier viruses often have the property that they can penetrate mucous membranes. So there is no need to inject them into the muscle with a syringe. In principle, they can also be put into a nasal spray, and on the mucous membrane, they enter the cells in the nose and develop their effect there. But at the moment we don't know anything about the side effects and this has to be looked at carefully. So we have to choose the same study order again. For many of these vector vaccines in humans, we do not yet have this mucosal experience, although we actually know from the animal model that this is what they provide."
Trials of several of the adenoviral vectored vaccines for nasal inhalation have already begun.
Thanks! This is very interesting.
Wouldn't this apply to other respiratory viruses? Does it?
Is influenza not "an infection of the mucous membrane" too?
There already exists such a nasal spray vaccine for influenza. And there is some hope for developing something like this for the common cold in the long run.
I have translated another part of the podcast mentioned above, about this subtopic:
"Christian Drosten: There are vaccines where this is already being done. For example, there is a nasal spray vaccine for influenza that can also be used in Germany. That is coming more and more. These mucous membranes, these nasal spray vaccines, are always genetically modified vaccines, i.e. carrier virus vaccines. This has not yet been recognized by the regulatory authorities long enough for it to be safe. Fifteen years ago, there were still great reservations about this, and today, with the increasing success of these carrier virus vaccines, especially in this SARS2 pandemic, these carrier virus vaccines are already quite successful in clinical trials. In the case of Ebola, they have been very successful. And now that more such good experiences are being made, it is to be hoped that more nasal spray vaccines will soon be available. And of course, this is then possibly also as an entry into a cold vaccination in the future. With the many cold viruses that we have, more than 15 viruses that can be listed, we may at some point come to a situation where we have nasal spray vaccines against almost all of them, especially for the adult population. So I think it is not unwise for the children to go through these harmless infections for certain immunological reasons. But for the adults these infections are in some cases anything but harmless. One has to imagine for the economy how many days of sick leave in an economy are caused by the whole bouquet of cold viruses every year. If one could vaccinate against them, that would be an incredible success."
Also, my boyfriend is an ICU nurse on the covid ward in a Southern state. He says average ICU stays are half as long now but that the average ICU patient is younger, so take that for what it's worth.
AstraZenica is piling on, their CEO previously saying they expect immunity from their vaccine to last a year. Article did not provide any explanation why they think it only lasts a year, but my guess is that this is merely more Doom Patrolling.
I don't think the statement that they expect a year worth of immunity is a statement that they believe it to not last longer then a year. Big Pharma companies are limited in what they can claim and if you are registering a 1-year clinical trial then it makes sense to speak about your expectation of 1-year worth of immunity.
I think that's reasonably chalked up as the work of Doom Patrolling even if it's not specific to this pandemic. But I expect you're right about the specific reasons for the one year duration.
Life had mostly returned to normal, masks were largely no longer being used at all.
I'm living in Berlin, which is a part of Germany with higher then average COVID-19 numbers and 160/100,000 cases at the time of me writing this comment.
I don't have the impression that people started wearing less masks. It seems to me that the primary change was the weather which drove people to spend more time indoors.
This matches my impression in Scotland. I also think there’s a fair amount of fatigue of following the rules so most people bend the rules slightly when it suits.
For the problem of vaccine trials ending prematurely, is it possible to setup a voluntary post-approval trial? Online registration and randomizing people to the control and treatment group seems easy enough, although you'd need to somehow get pharmacists on board if you want to do blinding (presumably pharmacists won't go along with it if they get a sealed letter asking them to inject the person in front of them with a saline solution). Unfortunately you probably need blinding, since people who know that they don't have a vaccine presumably act different than people who know they have a vaccine :\
Another option is a trial where everyone gets a vaccine. Each patient is randomized to get one of multiple vaccines. That should provide better evidence about the relative desirability of each vaccine. I'm pretty sure that we ought to want to focus on which vaccines are best, not on whether vaccines meet some pre-defined standard of effectiveness.
Alex Tabarrok has some related discussion in How to Vaccinate and Continue Clinical Trials.
I'm unclear why blinding is critical. It should have almost no effect on safety evidence. It seems likely to have a moderate effect on the quality of the efficacy evidence. But the harm from delaying vaccines for a few weeks seems a good deal larger than the harm from not having ideal information about which vaccine is most effective.
One of my biggest gripes with this whole situation is that I believe that if authorities treated us like adults, the ambiguity (COVID doesn't exist vs Very Serious People culture war) would be significantly mitigated.
What do I mean? I will use Ontario as a example.
On September 30th they came up with a modelling update.
https://files.ontario.ca/moh-fall-prep-modelling-deck-en-2020-09-30.pdf
Skipping to slide 9, I can infer very easily the following:
If we get to 150 COVID-19 patients hospitalized in the ICU, it starts becoming problematic for the health system in the province. If we get to 350, it starts breaking down the health system currently in place.
OK. Seems simple enough, where are we now?
https://covid-19.ontario.ca/data
As of today 77 people in the province are hospitalized in the ICU. I can also see that the number of COVID-19 ICU patients in August were between 11-30, in September from 12-35, and in October from 36-82.
Why is it that I had to do some decent Googling to find this information and come up with this conclusion? Why aren't government officials and the media telling us this information daily, so we as a population are aware that we are halfway in ICU hospitalizations for this to start becoming a problem, and thus we can personally adjust our behavior accordingly?
Authorities seem to think the masses are stupid, but then fail to do the bare minimum to educate them on the metrics that matter.
The sad thing is people are definitely smart enough to realize that just raw case numbers don't matter. But then they don't take the additional, and granted fairly tedious step, of figuring out which numbers do matter(hospitalization rates, positive test rates, death numbers, ICU usage rate in their area).
Or maybe it's pure red tribe blue tribe on a global scale(or rather with variations in different countries) and I'm being naive and hopeful.
Authorities seem to think the masses are stupid
I've found this to be much worse than just what you're claiming. Like how 'most people claim to be above average', I've noticed a lot of people claiming that most other people are stupid.
That's a really weird situation – a significant proportion of people think that almost everyone else can't handle hard truths (about whatever).
Or maybe it's pure red tribe blue tribe on a global scale ...
I think this is true, but in a weird 'fractal' number of dimensions beyond the obvious political coalitions. It's more like many-dimensional culture war than pure { red tribe / blue tribe } conflict, at least based on my own experience and personal observations.
We need more discussion of Slovakia's approach: Mass testing everybody with cheap antigen tests, testing is semi voluntary, if you don't have a negative test result you have to quarantine.
I maintain that the Slovak government has shown extraordinary competence here, when compared against an admittedly low international baseline. Even more astonishingly, the Lancet article makes it seem like they went against the advise of their scientific advisors who pushed for a 45 days lockdown.
- Before doing nationwide testing, they implemented a successful local test run.
- They understand what an incubation period is, and are therefore doing two runs, last weekend and this weekend.
- With antigen tests they settled for a good enough solution, understanding that they will catch the vast majority of infectious people who PCR tests would have caught as well.
- They managed to mobilize this whole initiative seemingly in a span of 2-3 weeks, with soldiers making sure distances are kept in waiting lines.
What I find most surprising is how discerning the government was in picking out the right advice and ignoring the bad scientific advice (at best governments follow one set of advisors completely, mostly they implement their recommendations in a worse than random way). Why bad? Because most epidemiologists only consider medical harm but not economic, and let the perfect be the enemy of the good:
The bad advice included: Antigen tests are less reliable than PCR tests, that there would be high infection risks at the testing sites, that not enough doctors would be available, that it would be immoral to forcibly quarantine people who do not want to be tested (apparently much better to effectively quarantine everybody in a lockdown), that a lockdown that would crush the economy was the better approach( what comes after the lockdown when the numbers will most likely rise again?)
This is not to say that each individual point was wrong or unlikely to happen, just that the epistemic standard when trying something new should not be "this will definitely work without any problems" but "this is worth a shot", particularly when the other alternatives have huge downsides as well. Neither am I saying that everything was done perfectly (I am unsure whether it is best to exclude 65+ citizens, citizens could maybe also do the swab testing supervised but themselves)
The jury is still out on whether this will flatten the numbers, but we should all hope that it works out for them so we have a viable alternative.
But on the question of whether the worst is behind us, the answer is probably yes.
This is underspecified. There are lots of ways that things could be bad.
In March and April, the hospital system broke down. Supply lines were hanging by a thread and we were having trouble finding ways to put literal food on our literal table, especially meat. Thousands were dying each day. Supply chains and the whole economy and the market on the verge of collapse. It’s easy to forget how bad things were at first.
OK, the disruption probably isn't coming back. But the deaths? You're predicting deaths shooting up; from current cases, I predict 1500/day. And how much higher will cases go? It's easy to imagine that they go up another 50% and deaths exceed previous rates. That's only about 2 weeks of growth at current rates. Why would they stop here?
I plan to address this next week in more detail but it's because I think IFR is low enough that we run into herd immunity first.
I'm talking about people infected in the next 2 weeks. I don't see how that is an answer unless we have already achieved herd immunity. And I'm skeptical that you can call the peak that precisely.
So what? There are individuals that have reached 100% infection. I'm talking about America, which is currently undergoing an epidemic. I'm predicting that the past 2 weeks of behavior will continue for the next two weeks. To predict otherwise on the grounds of herd immunity is to claim that it has been achieved just this week. Whereas, Qatar has steady levels, suggesting herd immunity in the current environment.
Qatar is believed to have reached more than half infected. Their median age is 30, however, which significantly mitigates the associated morbidity and mortality, as does the over 60 population being 2% of them compared to like 10% of the United States.
https://www.medrxiv.org/content/10.1101/2020.08.24.20179457v2
Same research finds only ~50 probable reinfections in a cohort of hundreds of thousands of followed individuals and all but one non-hospitalized and that one only out of caution.
Hmm, that paper references another paper for its >50% infected claim but the paper it references only has a 24% seropositivity rate. It does suggest 53.5% infection but that's based on a naive SIR model which I don't expect to give particularly accurate results for that kind of thing.
Good to see a detailed examination of reinfections though - that's the kind of thing I've been hoping to see.
Another, more recent, paper does find 66% seropositivity in migrant workers (who make up 60% of the population). However the sample seems to have been selected strongly for people who had had Covid as 20% of the sample had already had positive PCR results, compared to ~4% of the total population.
Good to see a detailed examination of reinfections though - that's the kind of thing I've been hoping to see.
User Annapurna posted a webpage that tracks Covid-19 reinfections, in case you hadn't seen it.
This cost of rules and restrictions seems highly underestimated. Rules and regulations crowd out a lot of private action. When we ask whether rules or private choices are most responsible for keeping us apart, don’t neglect the full extent to which rules crowd out that private action. Even without that, this new study finds private action is mostly responsible.
I thought this juxtaposition was interesting.
The Australian state of Victoria has recently emerged from an 111-day lockdown. On every one of those days, the state leader ("Premier") has fronted the media in a Cuomo-like press conference.
I think Zvi's skepticism about the proper role of government and the moral right of coercion has hardened into cynicism about leadership and state capacity being fundamentally insufficient to the task.
>We certainly are not going to allocate a scarce valuable resource according to ability to pay. That’s crazy talk.
Indeed, when talking about a vaccine that is crazy.
As an 'initial move' in the pandemic game, I sympathize with allocating-via-money as 'crazy'. But not doing that also has a significant opportunity cost long-term, e.g. foregoing resources for further production of vaccines that people want.
This is what 'public goods' with strong positive externalities provided by governments paying the vaccine companies are for.
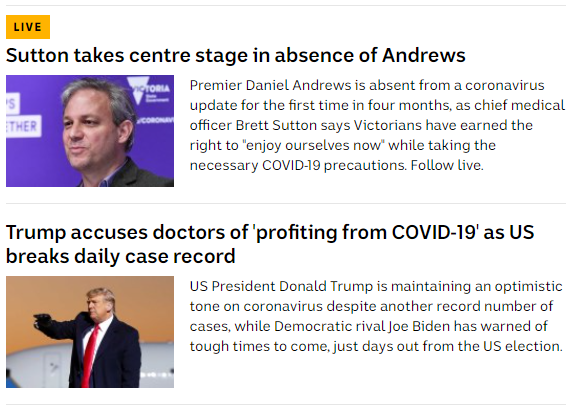
Trump wishes to register a complaint.
He does so within a thread full of clips that have to be seen to be believed but which you are under zero obligation to see either way.
Here is the central quote, which is real: “Covid, Covid, Covid, Covid, Covid, it’s all you ever talk about. A plane goes down, 500 people dead, they don’t talk about it. ‘Covid Covid Covid Covid.’ By the way, on November 4th, you won’t hear about it anymore … ‘please don’t go and vote, Covid!’”
This is his closing message to the American people. So unfair, we’ve beaten the virus, we’re turning the corner, we only have so many cases because we run so many tests. He kept saying it in the debate, he said it in the 60 Minutes interview, he says it rally after rally.
Whereas he now also claims that: “In California, you have a special mask. You cannot under any circumstances take it off. You have to eat through the mask. Right, right, Charlie? It’s a very complex mechanism. And they don’t realize those germs, they go through it like nothing.”
I mean, Covid is all we ever talk about here. That’s kind of the idea.
He must think these closing messages will resonate.
Most of all, Trump’s central point is he wants you to know that he is Not Biden, and most importantly, Not a Democrat. Because, you see, the Biden and the Democrats are terrible.
Meanwhile, Biden warns of a Dark Winter.
Biden also has a closing message. His closing message’s central point is clear. He wants you to know that he is most certainly Not Trump, and also Not a Republican. Because, you see, Trump and the Republicans are terrible.
Partisanship, as ever, is a hell of a drug.
As we discussed last week, two things are simultaneously true. Trump’s statements are completely unconnected to reality, and most the Doom Patrol of Very Serious People are also mostly unconnected to reality.
When it comes to Covid-19, both sides constantly make false claims about where things stand, with Trump’s claims being by far the farthest from reality.
But on the question of whether the worst is behind us, the answer is probably yes.
In March and April, the hospital system broke down. Supply lines were hanging by a thread and we were having trouble finding ways to put literal food on our literal table, especially meat. Thousands were dying each day. Supply chains and the whole economy and the market on the verge of collapse. It’s easy to forget how bad things were at first.
Yes, we might completely lose control of the situation once again. But thanks to improved treatments and mask use and all the time we’ve had to adjust and prepare, I don’t think there is room for things to be as bad as it was back then unless the medical system completely collapses. Barring a system collapse, we would get to herd immunity long before we got to 500k deaths.
Which is good, because White House Chief of Staff Mark Meadows said the quiet part out loud once again: ‘We’re not going to control the pandemic.’ This was a problem, because it undermines Trump’s message that the pandemic has already been controlled and will be gone any time now and he did a great job.
Vote. Consider everything you’ve seen, everything you’ve heard, and vote. In person or at a drop box. However long it takes. Pause here if you need to.
Then let’s run the numbers.
The Numbers
Deaths
The Midwest number is reassuring here, as it now looks like last week’s number was a bit of an aberration and got ahead of the curve. That doesn’t mean things are good, with clear increases in three of the four regions. We got to offset a lot of that because the South had a surprisingly good week for unclear reasons. While it makes sense that the South may improve in relative terms, as it is starting from a bad baseline and has warmer weather, it would be very surprising if things got actively better there any time soon.
Test Counts
We see substantially more tests than ever before, and also a full percentage point rise in the positive test rate. The problem is not only continuing, the problem is accelerating.
Positive Tests
This is why we shouldn’t expect the South to remain stable or improve. Like the other regions, cases are on the rise, and if anything that trend is accelerating rather than slowing down. For now only the Midwest region is setting all-time highs, but that is unlikely to last. The West should get there within a few weeks, with the South not that far behind, although the increased testing will obviously be some of that story. Either way, leading indicators this week seem to be consistent with the troubling end of the range of plausible outcomes.
Positive Test Percentages
(Note: Hawaii seems to have stopped reporting negative tests as of two weeks ago, I’m ignoring it because the size of the effect is so small.)
Again we have an unmistakable situation, with positive test rates rising across the board, even on rising test counts. Things are rapidly getting worse and there is no sign we are turning the corner. Nor does there seem to be any appetite for the type of response that would cause the corner to turn. It’s distressing to see this happen so close to a potential vaccine, but what remains of our civilization made its choices. Now it has to face the consequences.
That doesn’t mean a full-blown crisis or medical system collapse is inevitable. What we see here is consistent with an R0 of about 1.1. That means that we’d only need to cut our exposure by 10% to stabilize the situation, plus each day we get more help from herd immunity.
The question is whether colder weather and increasing fatigue, potentially combined with a loss of hope for containment, plus the messaging from Trump and supporters that the Covid-19 pandemic is effectively over, will make things worse faster than people’s control system reactions can bring things back in balance. The other question of course is whether there will indeed be any appetite to reapply meaningful restrictions, and enforce them enough that they are indeed meaningful. I don’t sense much eagerness to comply with official recommendations for Thanksgiving or Christmas gatherings, or on anything else that isn’t easy to enforce.
My advice is to assume that things are going to get substantially worse before they get better. Catching Covid-19 now is a lot less scary than it was back in April, but we might do substantial backsliding for a while on that front, and the risk of infection is high and growing higher. Prepare to have a lonely winter.
The good news for now is that deaths are still mostly under control, only up roughly 10%. This is the third week of cases rapidly increasing. If historical patterns continue, the next two weeks will see rapid increases in rates of death, and we’ll be able to fully confirm what is happening. If deaths do not see a rapid increase in the next two weeks, that will be a very surprising and hopeful sign, but it will only buy us a small amount of time.
I wonder to what extent people can ‘feel’ the danger levels rising. When they are told that things are rounding the corner and the virus is beaten, can they tell that this is not the case? Or is it mostly one set of talking heads saying one thing, while another set says another? At any given time, the number of infected is still relatively low, and they are clustered, so many won’t know anyone recently infected even if their social groups don’t wear masks or take many other precautions. For now, the hospitals are mostly holding together. A month or two from now at this pace, this will all be much harder to miss.
Note that it’s unlikely there will be a substantially safer time to do things, regardless of where you are located, within the next month and probably several months. If there are things you need to do, you’re better off doing them sooner rather than later. Same with people you want to see.
Europe
After asking around, the best data source that doesn’t require teeth pulling of any sort seems to be Our World in Data. One thing to be careful about is they only seem to get United States data with a few days of lag in some ways, so their test counts for us will take a while to become accurate.
So, how are things going out there?
Oh no.
Cases per million people:
Number of cases:
That’s over a 35% week over week increase, once again, for the European Union. The hockey stick is still shooting upwards. The United Kingdom is not as bad but still over a 10% increase. Both are running well ahead of the United States.
Here are positive test percentages:
And here are deaths:
France is off the charts for infections with deaths likely to soon follow, and is announcing a lockdown. Or at least, sort of:
If you are keeping schools open in light of the graphs above, and think you are not giving up, I don’t even know how to respond.
Not that giving up is obviously the wrong thing to do! But that does not seem to be Macron’s plan.
I got a lot of interpretations of what’s happening from European readers last week, all of which seemed mostly consistent. The model presented was that Europeans were under the impression that they had beaten the virus. Life had mostly returned to normal, masks were largely no longer being used at all. As the virus came back, governments wanted to keep the peace and thus chose to do nothing about it, and because they were told they’d won, the populations are not now willing to be told they need to lock down once more. There was little herd immunity being gathered over those months, so most everywhere was still highly vulnerable.
Essentially, Europe chose to declare victory and leave home without eradication, and the problem returned, first slowly, now all at once, as it was bound to do without precautions.
What I didn’t get from my readers were good (English language) news sources that could give me a feel for goings on across the pond that go beyond raw data. Suggestions on that are still appreciated.
Other Data Points
What other information did we get this week to help measure infection and death rates and how they are changing?
This is a good Twitter thread about France. Things have clearly been spiraling out of control there. He establishes that old people are not being protected, and expects to reach levels similar to the old peak 20 days out (at most 17 when you read this). He gives an estimate of R~1.2, which is lower than my instinctive guess which would be closer to R~1.35, but it’s possible. As usual, even when things look completely out of control, they aren’t that far from being turned around, if we cared enough. Some very good data analysis and visualizations later in the thread.
I don’t typically look too much at the numbers for hospitalizations, because who is hospitalized will be a function of availability of beds in which to be hospitalized and on various behavioral choices. I made that decision in April, when hospitals were at maximum in many places, making these problems severe. Also there were big data collection issues involved.
Still, one can reasonably say that they are a very good sanity or error check, and their relationships in time and magnitude to other factors can be enlightening:
The currently hospitalized line ran well above the new cases line in the first wave, despite the hospitals being maxed out. A lot of that is because our testing was also inadequate, but also our care has improved. In the second wave, the two lines are at similar levels. Now in the third wave, it looks like we are seeing concurrent hospitalizations running well below daily positive tests. The question is, to what extent is this lag, to what extent is this better testng, and to what extent is this better treatment or adjusting who we send to the hospital whether it’s better or not?
The linked article suggests about a 12-day lag between cases and hospitalizations. That seems long but plausible. If that’s the delay size, as the article notes, there has clearly been a divergence. Of course, they then warn that the virus is not less deadly, this is all due to other factors, because they are Very Serious People. Can’t win them all.
A different approach is to track Google searches, such as for loss of taste, and get this:
It doesn’t look good.
Also not looking good are the wastewater results from Boston (that link updates periodically).
I am not optimistic about that little tick down at the end being the new trend.
We also have reports that Utah hospitals are on the verge of rationing care, and temporary supplementary hospitals being deployed in El Paso. It’s getting bad out there.
Rule Abiding Citizen
My friend Luis reports that he has his bags packed because he is slightly outside the evacuation zone for the latest wildfire in Irvine, California.
There has to be some evacuation zone with some set of boundaries. The government has no choice but to say, those in this area must evacuate, and others must not.
But what do you do if you are slightly outside those barriers, presuming you think the government is making remotely reasonable choices?
You evacuate, of course. If it would be right to require you to take a safety measure if you were in slightly more danger, then you would be well-advised to take that measure now before things potentially get chaotic or out of control. This is the same principle that because I got my family out of New York City exactly in time, we were way too late.
Yet this is here because it is a clear example of how the opposite remains common. Once an evacuation zone is declared, the rule is not interpreted as telling one about the physical world so as to make better choices. The rule is that locations and behaviors inside this box are ‘unsafe’ because they are not allowed, and thus anything outside the box must therefore be ‘safe.’
Needless to say, this is madness.
If we do not think for ourselves, things will not go well.
It also points out a key danger when designing a rule. When telling people to stay six feet apart, you are preventing them from staying twelve feet apart. If you tell people gatherings are limited to ten people, many will think that means ten is fine. And so on.
It’s not that different from what happens when there’s a limit to how much chocolate cake you can eat, and you really should only eat about 75% of that amount. There is probably not going to be leftover cake.
This cost of rules and restrictions seems highly underestimated. Rules and regulations crowd out a lot of private action. When we ask whether rules or private choices are most responsible for keeping us apart, don’t neglect the full extent to which rules crowd out that private action. Even without that, this new study finds private action is mostly responsible.
All I Want For Christmas Is a Covid Vaccine
The Covid-19 vaccine hopefully will be ready soon. People will be lining up to get it and jockeying for priority so they can return to their old lives as soon as possible. There are tons of logistical and ethical issues to address to sort all that out.
We certainly are not going to allocate a scarce valuable resource according to ability to pay. That’s crazy talk.
Even crazier would be to not inoculate those in the placebo arm of the vaccine trials until the trials were over. You see, once there is an emergency use authorization allowing vaccination, things flip on a dime. Yesterday it would have been “unethical” and illegal to vaccinate anyone except in the test group of a controlled trial, no matter what they want. Today, it is “unethical” to not vaccinate the placebo arm of that same trial that is vital to knowing if our vaccine works. Thus, if we don’t confirm our effectiveness in elderly people first, we will never know, because otherwise finding out would be deeply “unethical”. As opposed to it being unethical not to know whether we are giving an effective vaccine to hundreds of millions of elderly people worldwide.
The people in studies that are gathering vital data must be given priority over a scarce resource, and vaccinated before others who need it, destroying our ability to gather data. As opposed to allocating the vaccine so as to run additional experiments and gather better data, or even just holding off on vaccinating those already providing invaluable data. Thank you once again, Copenhagen Interpretation of Ethics.
But that’s also only half the issue. That’s the half of people who realize that, at least once the scientists and regulations are onboard, getting a vaccine against a deadly virus is good.
What about the other half, who think that getting a vaccine against a deadly virus is bad? The people who don’t want it? There’s the anti-vax crowd. I’m sorry, they say, I thought this was America. There’s those who see the vaccine being approved while the other party is in charge, and don’t trust that. There’s those who think they can hold out and let other people try out the vaccine for them, and they’ll wait and see thank you very much, or even let those people eradicate the virus for them. There’s those who want to hold out until we know which vaccine is best, which of course we will never know because we won’t be allowed to run the necessary tests. There are those who are plain lazy.
They need a message given to them in a language they understand. They need a trustworthy and beloved fellow, an all-around jolly guy who they are used to using to get them to believe in the existence and benevolence of invisible forces beyond our understanding that don’t make any sense on reflection, and which we lie to our children about.
Who could be better for this job than our good friend Santa Claus?
Thus a planned $250 million government program to get mall Santas to advocate for vaccination (WSJ), which offered them an early place in line plus cash money to help convince the people to get the damn vaccine already once it was available.
People are treating this as another Trump mini-scandal and the latest horrible boondoggle. They are wrong. This is a great idea. The price tag is essentially zero dollars. Mall Santas are constantly in close contact with others, so giving them priority already makes sense. If people are going to take into their worldviews those who live at the North Pole and travel all around the world in one day delivering presents made by elves while keeping a list of which kids are naughty and nice? Yeah, it’s kind of weird. But let’s use that. What could be a better Christmas present?
This is an example of actually thinking and proposing something that might work. Even if it might have little or no effect, it’s definitely worth a shot.
Of course, once people heard about it, it was quickly cancelled. Previous versions were insufficiently explicit about this.
Doom Patrol
Good news! In an edit to correct a previous version of this post, Dr. Fauci has NOT thrown in with the eternally sacrificing scaremongers, who hereafter will be referred to as the Doom Patrol, by telling us that the vaccines will not block infection. I apologize to him and to all for the error. Instead, it is the headline writers and summarizers who took his true statement – that the vaccines are being tested and measured for preventing illness rather than testing for whether the person is infectious – and transformed that into “Dr. Fauci says early Covid vaccines will prevent symptoms, not block infections.”
That’s what the Doom Patrol does. It takes everything and uses it as a tool to show everything in the worst possible light.
The perversity of this resulting talking point is off the charts. It’s true that the vaccines might not block infection, but there is no scientific reason to assume that they wouldn’t. Nor is there any reason to draw the conclusion these headlines are effectively designed to cause people to draw, which is that someone with the vaccine is still potentially infectious and should not be treated as safe.
Then there’s the social implications of this line of rhetoric, taken purely as a consequentialist attempt to change behaviors. They’re pushing the line that even after both of you have an effective vaccine you still need to socially distance. The implication is that our lives will never return to normal, or would only do so after eradication.
This kind of willful misinterpretation is the norm. It works. It gets clicks, and it gets rewarded. I fell for it too, and I’m sorry about that, and thankful to those on Twitter who found and corrected my mistake.
I don’t think this is something being said in order to influence behavior, or even to influence beliefs. That is not the mindset we are dealing with at this point. It’s not about truth. It’s not about consequentialism. We have left not only simulacra level 1 but also simulacra level 2 fully behind. It’s about systems that instinctively and continuously pull in the direction of more fear, more doom, more warnings, because that is what is rewarded and high status and respectable and serious and so on, whereas giving people hope of any kind is the opposite. That’s all this is.
Doom Patrol Warnings
Now Look What You Made Me Do is a favorite of the Doom Patrol. We are going to lock you down if you misbehave, so if you misbehave all you’re doing is locking yourself down. She’s right, of course, that things will keep getting worse until we change the trajectory and make them start getting better, but no the interventions to regain control are exactly the same either way. You either get R below 1, or you don’t. Except that the more it got out of control first, the more voluntary adjustments you’ll see, and the more people will be immune, so the more out of control it gets the easier it is to control later.
Another favorite is the Nightmare Herd Immunity Multiplication. You get claims like this:
Which is one of the better ones, since even though I think we’re past 15% infected, 15% isn’t a crazy estimate, and he didn’t pretend it was only the 2.6% that have had a positive test. But he ignores the obvious point that the infection fatality rate is far, far lower. If we’re at 15% infected with 223,000 deaths including the period where CFR was 1% or more, and it’d down by at least a factor of three, then no, we can’t have another 500,000 deaths. There’s only 85% of the population left, by your own estimate, and to get to a ‘lower bound estimate of herd immunity’ there’s a lot less than that. We mathematically have to be more than halfway done in terms of deaths unless the medical system collapses.
It seems every week I feel forced to reiterate that it’s been one more week without substantial numbers of reinfections, thus pushing our best guess for how long immunity lasts to two weeks longer than before due to the Lindy rule. That’s because every week we get warnings about how immunity is temporary.
AstraZenica is piling on, their CEO previously saying they expect immunity from their vaccine to last a year. Article did not provide any explanation why they think it only lasts a year, but my guess is that this is merely more Doom Patrolling. The vaccine is great if it has to be retaken every year, so long as it works, so no reason not to look like a responsible Very Serious Person and give your lower bound estimate as your overall estimate.
This of course comes from a story that their vaccine produces immune response in children and in both younger and older adults. That doesn’t mean it works, but it’s a very good sign. So we’d better find some downside to remind our readers of as well, lest they have some hope.
Similarly, a useful investigation into whether a new virus variation is more infectious than the old one is explicitly said to not be useful, because either way you should be afraid of the virus, and you should never take anything else away from scientific information. If the virus is confirmed to have become more infectious, that provides a huge hint in figuring out what is going on, and changes our calculus. The more infectious the virus is, the more we need to either do a better job containing it, or decide that it’s not worth containing. And the more we can get a realistic assessment of how effective our various countermeasures have been in containing spread. You need to know the baseline. Also, it notes that full cross-immunity holds, so you don’t have to care about which one you are exposed to or catch in that sense.
Covid-19 Ages Brains Ten Years, Says Doom Patrol
A paper came out last week where they administered an intelligence test to those who had recovered from Covid-19 in the United Kingdom, and found substantial negative effects on cognition even for those who had not experienced major symptoms. I didn’t get to the paper last week, so I’m looking at it now.
This paragraph jumped out at me:
Participants | Amongst 84,285 participants, 60 reported being put on a ventilator, a further 147 were hospitalised without a ventilator, 176 required medical assistance at home for respiratory difficulties, 3466 had respiratory difficulties and received no medical assistance and 9201 reported being ill without respiratory symptoms. Amongst these 361 reported having had a positive biological test, including the majority of hospitalised cases.
That’s really weird, right? We have only 361 ‘positive biological tests’ out of about thirteen thousand participants reporting having Covid-19. So only three percent of them had a positive test at all? I suppose we should be grateful for what little testing we have here in America!
Here’s their core finding:
The scale of the observed deficits was not insubstantial; the 0.57 SD global composite score reduction for the hospitalised with ventilator sub-group was equivalent to the average 10-year decline in global performance between the ages of 20 to 70 within this dataset. It was larger than the mean deficit of 512 people who indicated they had previously suffered a stroke (-0.40SDs) and the 1016 who reported learning disabilities (-0.49SDs). For comparison, in a classic intelligence test, 0.57 SDs equates to an 8.5-point difference in IQ. At a finer grain, the deficits were broad, affecting multiple cognitive domains.
Here’s the core results graph:
Here is that split up by task:
The effect size for those not hospitalized seems small, on the order of one or two IQ points. A substantial life disruption combined with various subtle selection effects seems like it should be enough to account for this. When one is coming off a serious health scare it can be tough to focus and think straight.
Their take is this:
Previous studies in hospitalised patients with respiratory disease not only demonstrate cognitive deficits, but suggest these remain for some at a 5 year follow-up 19. Consequently, the observation of post-infection deficits in the subgroup who were put on a ventilator was not surprising. Conversely, the deficits in cases who were not put on a ventilator, particularly those who remained at home, was unexpected. Although these deficits were on average of small scale for those who remained at home, they were more substantial for people who had received positive confirmation of COVID-19 infection.
It seems that it takes a lot to get confirmation out of the UK medical system. This raises the question of how those who had few or no symptoms could know they have Covid-19 without a positive test, which suggests that they’re using terms in strange ways.
The bottom line question is, should you be afraid for your own cognition?
My reply would be essentially no. These effects are large for those coming off respirators, sure. But they’re much smaller than the IQ deficit I and likely most of you are suffering due to worrying about Covid-19, or the one from us worrying about politics, or any number of other similar things. I don’t think we have to worry about this as a physical risk.
Thus I do not think that this finding should adjust our priors much on how much we should care about not catching Covid-19.
Of course, when the Doom Patrol gets hold of such findings, they get misrepresented. Even places like The New York Post end up telling their readers things like: COVID-19 causes ‘chronic’ cognitive deficits equivalent to brain aging 10 years without clarifying that this is only for the patients who were on ventilators. If you read that article, or you look at crazy headlines like this…
…you would come away with the impression that the problem is an order of magnitude worse than the paper claims.
Bursting Your Bubble
In the seventh inning of the sixth and final game of the World Series, which was played in a bubble in Texas, Justin Turner of the Dodgers was taken out of the game. Baseball later revealed that this was due to him having had a positive Covid-19 test, after having been told that his previous test was ‘inconclusive.’
When the Dodgers won the game and with it the World Series title, Justin Turner joined his teammates for an on-the-field celebration, including what definitely qualifies as a lot of close contact.
That did not make any more sense than it did in your head.
Baseball, it seems, runs its tests on players during games. This would seem to be rather useless, or at least epically bad timing. Isn’t the whole point to test you before the game so you can not play if you’re positive? One would think so. And somehow there was previously an ‘inconclusive’ test, and it took them until the eighth inning to clarify? Which given it was playoff baseball, means presumably a bare minimum of three hours.
That pales in comparison to the post-game celebration. What the hell is he doing on the field doing a traditional post-victory celebration? Isn’t that going to infect the whole team?
Well, yeah, good chance of that. Yet it was allowed to happen anyway.
You can call Turner selfish, or his team foolish, and like MLB throw Justin under the bus. You could also plan on lumping the Dodgers in with the Astros and debating whether it’s better to infect your whole team or to illegally steal signs. It’s certainly a valid perspective.
But you know what else is a valid perspective? He just won the damn World Series.
This is the moment Justin Turner and the Dodgers have been working for their entire lives. There is a good chance, as good as the Dodgers are, that it will never happen for him again.
Is it so crazy to think that, given the risk level for healthy ballplayers in their 20s and 30s at this point in the pandemic, and an entire offseason to recover, that maybe let them all have this moment?
I don’t think there’s a right or wrong answer. But that’s the point. Life is always about tradeoffs. Life under Covid-19 even more so. Certainly I would have tried to celebrate in less obviously risky ways on the margin than what happened, if at all possible. But no. I don’t think celebrating with the team was a horrible decision. Life matters. The highlight of your life, that so many dream about and few achieve? That really matters.
It’s certainly plausibly a lot less crazy than when I stood in a line of people for an hour on Tuesday, in the middle of a pandemic, so that I could take the purely symbolic step of voting in New York. Which don’t get me wrong, I’m happy I did, but imagine dying to ever so slightly change numbers that are in no way in doubt and that no one will ever look at.
Transmission Risk Explained Pretty Darn Well
As these things go, this explainer about how various decisions influence Covid-19 infection risk is quite good. It comes off as way too confident, and even more than that too definitive about what outcomes will happen. This transforms an ‘on average’ result into a resounding inevitable victory for karmic justice. Even more than that, they seem to conflate some sort of ‘up to X infected’ with ‘definitely X infected,’ which is far more misleading than conflating with ‘an average of X infected.’ Perhaps people need to hear that. I think it is more likely that the Very Serious People only think people need to hear that, but I understand their perspective.
The big thing this emphasizes, that almost everyone neglects, is the importance of airflow. If one must be indoors for an extended period, it is vital to avoid poor ventilation. Masks are great, keeping social distance in the moment is great, but you also need to open a window and ideally do much more than that.
Every time I see explanations like this, once I set aside my urge to nitpick, the thing that always strikes me is that it’s kind of hard to catch Covid-19. Yes, if you talk to people in indoor spaces for long periods with people who are infected, it won’t be long before you catch it. But if you’re taking reasonable precautions, together those precautions drop your risk by orders of magnitude. Your chances are pretty damn good.
In Other News
We now have a new case of reinfection, because someone deliberately reinfected themselves. I am willing to acknowledge that if you actively try to get infected a second time, it can work, so immunity is not total and permanent. We still await seeing substantial reinfections. On the flip side, CNN reports that a new study finds that immunity lasts for at least five months, and the title of the study was for some reason not ‘we paid a tiny amount of attention to the world.’
Antibody treatments work but are hard to make and therefore expensive. Several companies are working on them. Regeneron reports its cocktail is highly effective, but that it only has about 50,000 doses worth of treatment available at this time. The government agreed to pay them about $150 per dose, which seems like a bargain at ten times the price.
Flu shots correlate with less Covid-19 infection. I’d be very careful ascribing this to causation, but the effect size is rather large.
AstraZeneca is allowed to resume its American vaccine trial that was halted due to a death in the placebo group, weeks after its other trials resumed. So naturally the move is to complain about a lack of transparency.
Masks do seem to correlate quite well with reporting of symptoms. What a coincidence. Of course, common cause is still a plausible explanation if you want to explain this away. Or you could find something else with a R-squared of 0.73 and mock the results. Either way.
Twelve minute naval swab test coming to United Kingdom pharmacies. I’m cautiously hopeful, but we keep hearing about such things and then they mostly don’t materialize or don’t happen in large numbers. As I’ve said multiple times, this is a huge step forward and a potential Path to Victory on its own.
A prison might not be the safest place to catch Covid-19.
Should vaccination prioritize the most vulnerable, or those who could resume the most valuable economic activity? Here is one attempt at an answer that says it depends on the counterfactual that would have happened with no vaccine. I applaud this person for at least trying to think about this, even if what resulted was mostly nonsense. No one seems to have pointed out that his line of reasoning makes actual zero sense. The counterfactual is the other prioritization option. You have two worlds, you choose between them based on which is better. What the world would be if you didn’t choose either option doesn’t matter at all.
Don’t Mention the War
This Tuesday is Election Day.
Remember that there is a good chance we won’t know the winner on election night, or even if we essentially know, that we won’t be able to call the race let alone get a concession.
It is probable but far from certain that Trump will lose and then refuse to admit defeat. He will almost certainly fight in the courts to the extent available. He may do more than that. There may be serious attempts to prevent votes from being counted, or to disregard them despite the count. Be mentally prepared.
There is even a small but real chance that there will be substantial disruptions or even violence in the wake of the election.
It is far from the top of the list of concerns raised by such possibilities, but it is also true that all of this could make the Covid-19 situation much worse.
Be physically and mentally prepared to deal with all of that. It probably will all be fine, the same way that catching Covid-19 will probably not kill you. But either way, best to be prepared.
If we are all fortunate, by the time I sit down to write my November 5 column, we will be able to dismiss all these concerns and get back to worrying about Covid-19. The Covid-19 news is unlikely to be good next week, but if we are properly calibrated then in that sense good news is always a strong possibility.
In the meantime, vote, and maybe also try to convince others, and prepare as need be, but also do whatever you need to do to not stress out about the election and get through the coming week. Stressing out and doomscrolling, or posting on social media to make others stress out, does not do anyone any good, no matter what outcome you prefer. You have full permission to eat delicious desserts, play games, get it on, aggressively use counterprogramming that lacks any redeeming social value, and do whatever else you find helps keep you safe and sane. Treat yourself.
It’s been a long year. You’ve earned it.