Introduction
One of the main places Americans look for information on coronavirus is the Center for Disease Control and Prevention (abbreviated CDC from the days before “and Prevention” was in the title). That’s natural; “handling contagious epidemics” is not their only job, but it is one of their primary ones, and they position themselves as the authority. At a time when so many things are uncertain, it saves a lot of anxiety (and time, and money) to have an expert source you can turn to and get solid advice.
Unfortunately, the CDC has repeatedly given advice with lots of evidence against it. Below is a list of actions from the CDC that we believe are misleading or otherwise indicative of an underlying problem. If you know of more examples or have information on any of these (for or against), please comment below and we will incorporate into this post.
Examples
Dismissed Risk of Infection Via Packages
On the CDC’s coronavirus FAQs pages on 2020-03-04, they say, under “Am I at risk for COVID-19 from a package or products shipping from China?”:
“In general, because of poor survivability of these coronaviruses on surfaces, there is likely very low risk of spread from products or packaging that are shipped over a period of days or weeks at ambient temperatures.”
However, this metareview found that various coronaviruses remained infectious for days at room temperature on certain surfaces (cardboard was not tested, alas) and potentially weeks at lower temperatures. The CDC’s answer is probably correct for packages from China, and it’s possible it’s even right for domestic packages with 2-day shipping, but it is incorrect to say that coronaviruses in general have low survivability, and to the best of my ability to determine, we don’t have the experiments that would prove deliveries are safe.
Blinded Itself to Community Spread
As late as 2020-02-29, the CDC was reporting that there had been no “community spread” of SARS-CoV-2. (Community spread means that the person hadn’t been traveling in an infected area or associating with someone who had). At this time, the CDC would only test a person for SARS-CoV-2 if they had been in China or in close contact with a confirmed COVID-19 case.
Testing Criteria as of 2020-02-11
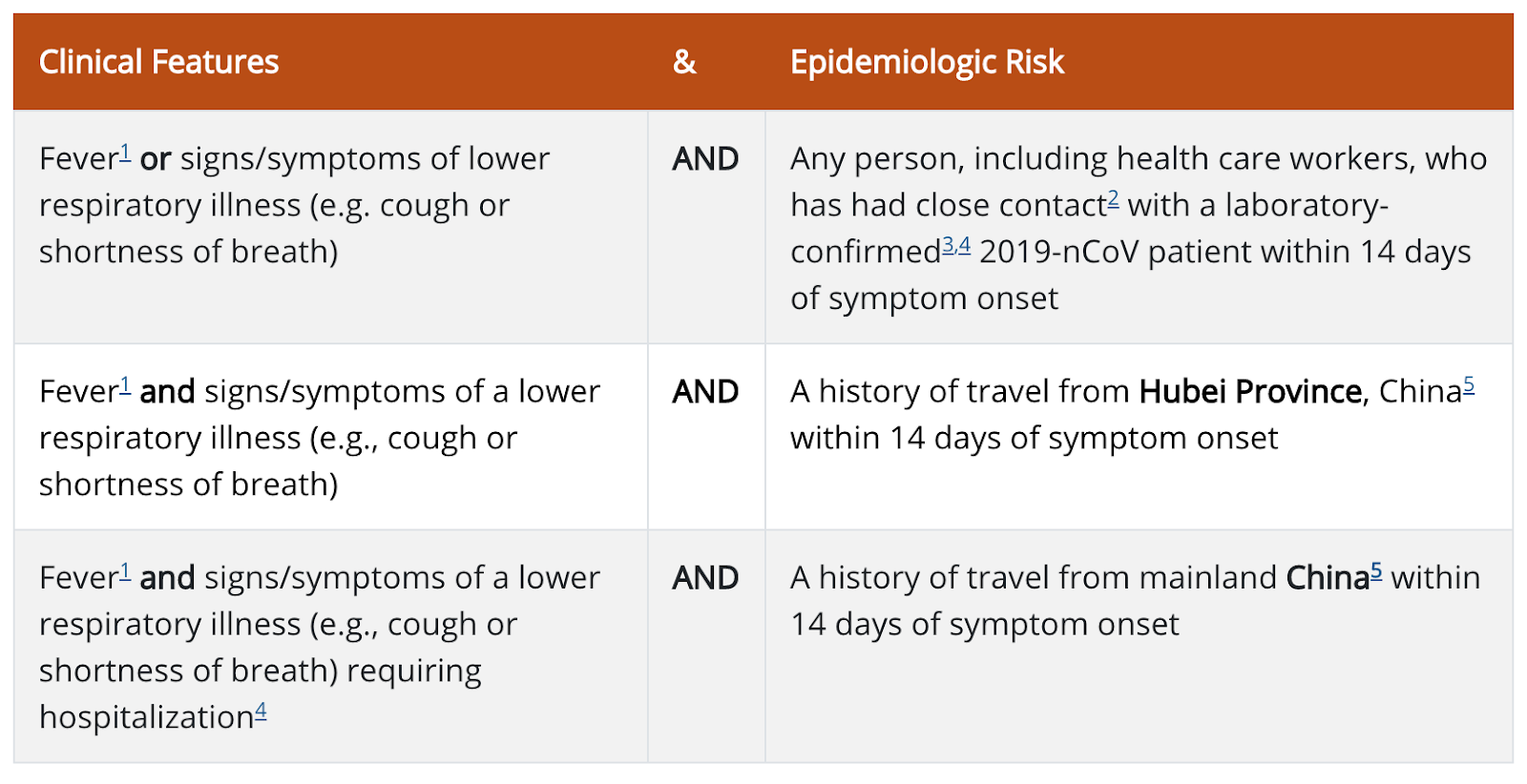
This not only left them incapable of detecting community spread, it ignored potential cases who had travelled to other countries with known COVID-19 outbreaks.
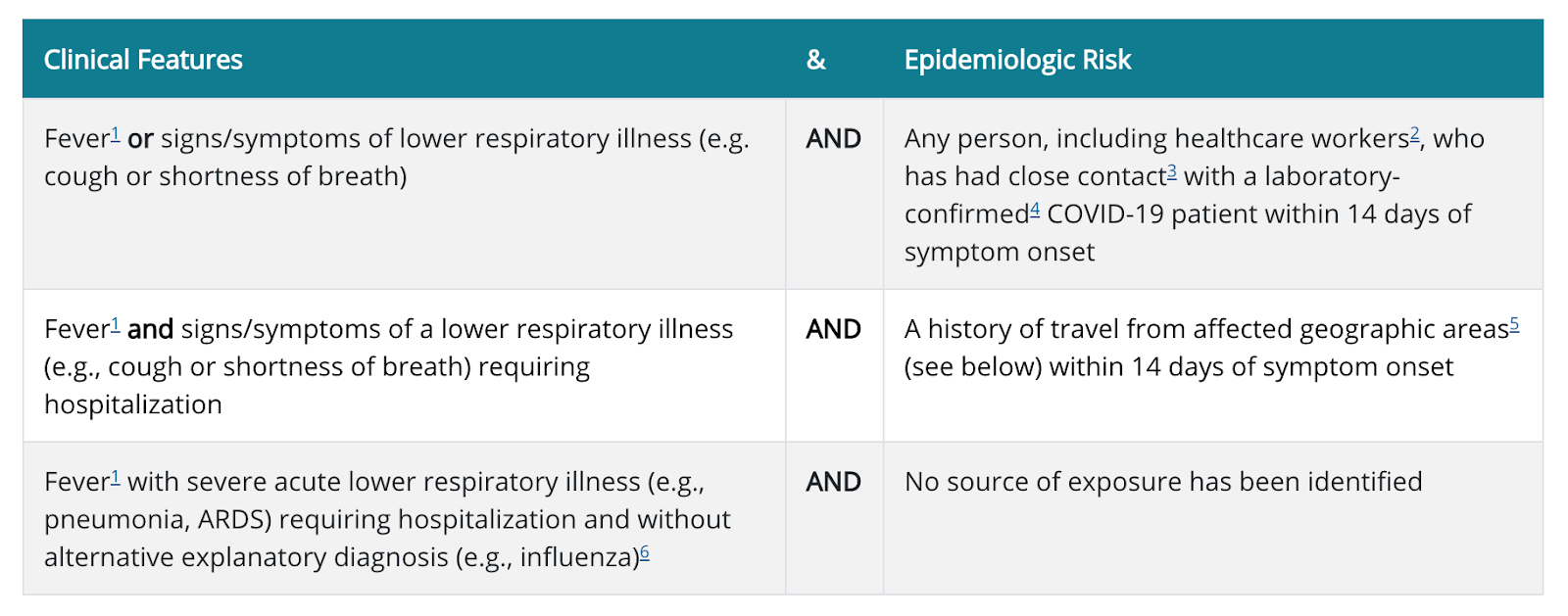
By 2020-02-13, this had been amended to include
The criteria are intended to serve as guidance for evaluation. Patients should be evaluated and discussed with public health departments on a case-by-case basis. For severely ill individuals, testing can be considered when exposure history is equivocal (e.g., uncertain travel or exposure, or no known exposure) and another etiology has not been identified.
(The CDC describes this change as happening on 2020-02-12, however the Wayback Machine did not capture the page that day).
Based on this announcement on 2020-02-14, when testing that could detect community exposure was happening it was in one of 5 major cities. However as of 2020-03-01 only 472 tests had been done, so no test could have been happening very often.
Between 2020-02-27 and 2020-02-28, the primary guidelines on this page were amended to
However guidance went out on the same day (the 28th) that only listed China as a risk (and even then, only medium risk unless they had been exposed to a confirmed case or travelled to Hubei specifically).
Testing Kits the CDC Sent to Local Labs were Unreliable
They generated too many false positives to be useful.
Hamstrung Detection by Banning 3rd Party Testing (HHS/FDA, not CDC)
One reason the CDC used such stringent criteria for determining who to test was that they had a very limited ability to test, hamstrung further by the faulty tests sent to local labs. Normally private testing would fill the gap, but the department of Health and Human Services invoked emergency measures that created a requirement for special approval of tests, and the FDA didn’t grant it to anyone (source).
There are multiple harrowing stories of people with obvious symptoms and exposure to the virus being turned away from testing, often against a doctor’s pleas:
- UC Davis patient
- NYC ER doctor complains about inability to test
- NYC man returning from Japan
- Northern California nurse who treated infected patient
There is also a rumor that the first case caught in Seattle, which has since turned into the US epicenter of the disease, was caught by a research lab using a loophole to perform unauthorized testing (raising the possibility that it’s worse elsewhere and simply hasn’t been caught).
Ceased to Report Number of Tests Run
Until 2020-03-02, the CDC reported how many tests SARS-CoV-2 tests it had run. On March 2nd, it stopped (before, after). There are many potential reasons for this, none of which inspire confidence. The official reason for this as told to reporter Kelsey Piper is that the number would no longer be representative now that states are running their own tests. So, best case scenario, the CDC can not coordinate enough to count tests performed by other labs.
Gave False Reassurances About Recovered Individuals
As of this writing (2020-03-05), the CDC’s “Share Facts” page states that “Someone who has completed quarantine or has been released from isolation does not pose a risk of infection to other people.”
While it is certainly true that being released from quarantine implies a significantly reduced risk, the quarantine that is typically performed is not stringent enough to say that people released pose no risk. The quarantine procedure performed by the CDC lasts 14 days, after which if symptoms have not appeared, they can be released.
There are case reports of individuals with incubation periods of 27 days and 19 days. There was a case in Texas where a person tested positive after being released from quarantine and visiting a mall.
While an epidemic is still contained, safely quarantining at-risk people means choosing a quarantine period long enough to be confident that, if they haven't shown symptoms, they don't have the disease. When a disease is still contained, this should be risk averse, since a single infected person could start an outbreak. The CDC's 14-day quarantine period was not long enough to catch the cases detailed above.
This was foreseeable. This paper, published Feb 6, estimated the distribution of incubation periods, including the incubation periods of outliers.
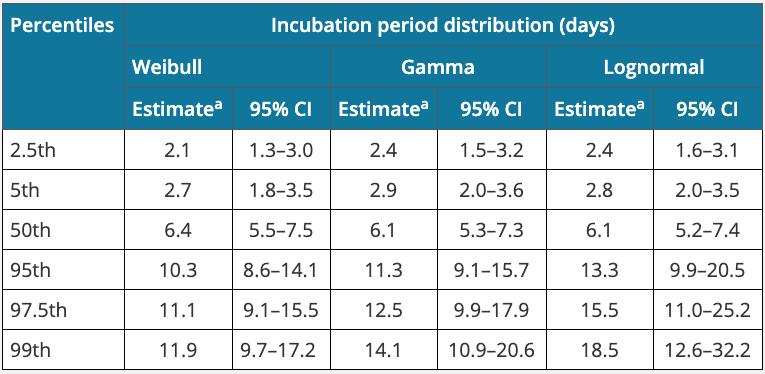
The relevant row is the 99th percentile row, which estimates the longest incubation period per 100 people. If you quarantined 100 people, one of them would have an incubation period at least that long. The paper estimates this using three different methods; two of those estimates are greater than 14 days, and all three estimates put significant probability on incubation periods longer than 14 days.
There are also reports of the virus re-emerging in patients who were believed to have recovered.
Conflated Genetics and Environmental Exposure
This is a tough topic to write about.
Cruelty to people because they have or might have a disease is never okay. And the vast majority of people who were cruel to Asian-appearing people in the early days of an epidemic were doing it to healthy people out of knee jerk fear and antagonism, not a measured, well-informed cost-benefit analysis. When the CDC claimed on 2020-02-29 that "People of Asian descent, including Chinese Americans, are not more likely to get COVID-19 than any other American." they were surely trying to dampen attacks on people who had done nothing wrong and were hurting no one.
But the statement is false. Chinese-Americans are more likely to travel to China or associate with people who have, and thus were more likely to catch SARS-CoV-2. This doesn’t mean they are more likely to catch it given exposure, but they were more likely to be exposed.
The CDC admits this in the page specifically on stigma (2020-02-24), saying “People—including those of Asian descent—who have not recently traveled to China or been in contact with a person who is a confirmed or suspected case of COVID-19 are not at greater risk of acquiring and spreading COVID-19 than other Americans.”
However that same anti-stigma page goes on to say “Viruses cannot target people from specific populations, ethnicities, or racial backgrounds.” This is also false. About 10% of Europeans are immune to HIV, an immunity not found people originating from other areas. So we know it is technically possible for a virus to have differential effects based on race.
Does SARS-CoV-2 in particular have race-related effects? There are people claiming Asian men are more susceptible to SARS-CoV-2 than others due to a higher expression of a certain protein (example). Other people dispute this (example). Right now it is very much an open question.
We can see why the CDC prioritized calming racially-motivated violence over fully explaining their confusion over an unanswered question. It might have been the highest-utility thing to do. But it is important to know that “misrepresenting data in order to produce better actions from the public” is a thing the CDC does.
Discouraged Use of Masks
Which brings us to the CDC’s statement on masks:
CDC does not recommend that people who are well wear a facemask to protect themselves from respiratory diseases, including COVID-19.
The Surgeon General (who is not directly part of the CDC) takes a stronger tack:

While we can’t hold the CDC responsible for the Surgeon General, they are being conflated in a lot of news articles saying or implying that masks are useless for healthy people. They’re (probably) not.
Our best guess is that the CDC is trying to conserve masks for health care professionals and others with the highest need, in the face of a looming mask shortage. That could easily be the optimum mask allocation. I can’t prove the lie wasn’t justified for the greater good. But it is another example of the CDC placing “getting the outcome it wants” over “telling people the literal truth.”
What Does This Mean?
These errors we’ve highlighted tend towards errors of omission: saying something is completely safe when it’s not, saying something is unhelpful when it is, saying the current state is less dangerous than it is. You should include that bias when processing new information from the CDC. Notably we’re not saying any of the things they do recommend are bad: to the best of our knowledge, you should be washing your hands and not touching your face. Vaccines are (mostly) great. But I would not take the CDC saying an activity is safe or unnecessary as the last word on the subject.
I want to apologize, and make sure there is a clear record of what I think both on the object level, and about my comment, in retrospect. (For other mistakes I made, not related to this comment, see here.)
I handled this very poorly, and wasted a significant amount of people's time. I still think that the claims in the post were materially misleading, (and think some of the claims still are, after edits.) The authors replaced the section saying not to listen to the CDC with a very different disclaimer, which now says: "Notably we’re not saying any of the things they do recommend are bad." I think we should have a clear norm that potentially harmful things need a much greater degree of caution than it displayed. But calling for it to be removed was stupid.
Above and beyond my initial comment, critically, I screwed up by being pissed off and responding angrily below about what I saw as an uninformed and misleading post, and continued to reply to comments without due consideration of the people involved in both the original post, and the comments. This was in part due to personal biases, and in part due to personal stress, which is not an excuse. This led to what can generously be described as a waste of valuable people's time, at a particularly bad time. I have apologized to some of those those involved already, but wanted to do so publicly here as well.
Reviewing the arguments
I initially said the post should have been removed. I also used the term "infohazard" in a way that was alarmist - my central claim was that it was damaging and misleading, not that it was an infohazard in the global catastrophic risk sense that people assumed.
Several counterarguments and response to my claim that it should be taken down were advanced follow. I originally responded poorly, so I wanted to review them here, along with my view on the strength of the claims.
1) I should not have been a jerk.
I was dismissive and annoyed about what seemed to me to be many obvious factual errors. My attitude was a mistake. It was also stupid for a number of reasons, and at the very least I should have contacted the authors directly and privately, and been less confrontational. Again, I apologize.
2) Telling people to check with others before posting, and threatening to remove posts which were not so checked, is censorship, which is harmful in other ways.
As I mentioned above, saying the post should be removed was stupid, but I maintain, as I did then, that when a person is unsure about whether saying something is a good idea, and it is consequential enough to matter, they should ask for some outside advice. I think this should be a basic norm, one that lesswrong and the rationality community should not just recommend but where feasible, should try to enforce. I do think that there was a reasonable sense of urgency in getting the message out in this case, and that excuses some level of failure to vet the information carefully.
3) We should encourage people to say true things even when harmful, or as one person said "I'd want people to err heavily on the side of sharing information even if it might be dangerous."
This stops short of Nietzschean honesty, but I still don't think this holds up well. First, as I said, I think the post was misleading, so this simply does not apply. But the discussion in the comments and privately pushed on this more, and I think it's useful to clarify what I claimed. I agree that we should not withhold information which could be important because of a vague concern, and if this post were correct, it would fall under that umbrella. However, what the post seem to me to try to do is collect misleading statements to make it clearer that a bad organization is, in fact, bad - playing level 2 regardless of truth. That seems obviously unacceptable. I do not think lying is acceptable to pursue level 2 goals in Zvi's explanation of Simulacra, except in dire circumstances.
But the principle advocated here says to default to level 1 brutal / damaging honesty far more often than I think is advisable, not to lie. My initial impression what the the CDC was doing far better than it in fact was, and that the negative impacts were greatly under-appreciated.
I can understand why the balance of how much truth to say when the effect is damaging is critical, and think that Lesswrong's norms are far better than those elsewhere. I agree that the bare minimum of not actively lying is insufficient, but as I said above, I disagree with others about how far to go in saying things that might be harmful because they are true.
4) We should not attempt to play political games by shielding bad organizations and ignoring or obscuring the truth in order to build trust incorrectly.
I think this is a claim that people should never play level 3. I endorse this. I agree that I was attempting to defend an institution that was doing poorly from claims that it was doing poorly, on the basis that a significant fraction of those claims were unfair. As I said above, this would be a defense. In retrospect, the organization was far worse than I thought at the time, as I realized far too late, and discussed more here. On the other hand, many of the claims were in fact misleading, and I don't think that false attacks on bad things are OK either.