Repost from wordpress blog
status rapport from Denmark
Key numbers: they give numbers of cases by day, and also give cases of omicron as a percentage of other cases.
Of 785 cases in Danish citizens, 76.31% of omicron cases where in double vaxed, 7.13% in triple vaxed, compared to 73.69% double (probably also including triple) vaxed for covid in general. 14.14% unvaxed for omicron 22.93% for general (over the last 7 days)
Rate of hospitalization is 1.15% for omicron (9 cases), and 1.85 in general.
Everything is probably confounded by age and region. (omicron is less prevalent in children and over 65)
sources: https://experience.arcgis.com/experience/aa41b29149f24e20a4007a0c4e13db1d/page/page_5/ https://files.ssi.dk/covid19/omikron/statusrapport/rapport-omikronvarianten-09122021-ke43
Updated numbers from today at: https://files.ssi.dk/covid19/omikron/statusrapport/rapport-omikronvarianten-10122021-ek56
Now with English translations.
Only significant change is that hospitalizations are up to 1.4% (18 cases).
There should be daily updates found her https://www.ssi.dk/aktuelt/nyheder/2021
click the newest one and click "læs rapporten her" (read the report here). Which takes you to a page where you can download the rapport for that day
Regarding the false headline ("'almost certainly' less severe"): I googled it to check the details, and it turned into a spot check of headline-writing honesty/competence among media outlets. Thankfully most went with "Omicron 'almost certainly' not more severe than Delta, says Fauci", which is what he actually said:
On the question of severity, "it almost certainly is not more severe than Delta," said Fauci.
(https://www.france24.com/en/live-news/20211207-omicron-variant-almost-certainly-not-more-severe-than-delta-fauci-tells-afp)
Can immune escape by itself explain the transmission advantage or do we also need it to be spreading better?
In theory if enough people have enough immunity you can explain any advantage with immune escape. I can't rule it out. However, I'm skeptical, primarily because if everyone was previously infected then you wouldn't see vaccines giving much advantage vs. infection (either by Omicron or Delta) or protection against severe disease. The fact that vaccines or being infected still matters vs. baseline population puts a not-too-high cap on how many people have already been infected, which in turn makes the current doubling times very hard to explain with evasion alone.
Trevor Bedford gets into this, and the short answer is technically yes, but the important part about decomposing Rt is not the decomposing it per se but the info it yields on how much vaccine escape might be going on. For reasonable R0s, there has to be substantial vaccine escape. https://twitter.com/trvrb/status/1466076797670363140
Regarding translating fold reductions of neutralization titers into vaccine effectiveness, I always go back to this: https://www.nature.com/articles/s41591-021-01377-8 (Fig 1a). Titers ~4x convalescent is what mRNAs do against wild-type, getting them to about 90%+ efficacy. About a 2x reduction against Delta means titers ~2x convalescent, getting them to about 85% efficacy. These conform with what we've seen. A 25-40x reduction against Omicron means titers .10-.16x convalescent, getting us down to 40% efficacy for two shots. Pfizer says a booster gets us back to "full" efficacy, and hopefully that holds up!
Connecting omicron and your previous post on R0, is it possible that a significant reason for the increase in effective infectiousness for omicron is that the people with higher individual R0 are now back in the susceptible population due to the significant immune erosion?
I think the default assumption is that everyone is back in the pool of potential infections, which is yet one more reason to think that it will get out of hand quickly at first.
I forgot how priceless that SNL skit was. Thanks for the excuse to re-watch it. I love when they break character - it just works.
"Are you OK, Kate?"..."Obviously I'm not"
The London School of Hygiene released a modelling paper describing some estimated effects on the UK of the Omicron wave. Mostly, it's a lot of "the error bars on all these are giant, and we don't have any clear idea what's going to happen except that there will be a giant wave of infections by mid-Jan, unclear how that translates to deaths".
If you assume no new measures and no behaviour change in the UK, you get a ridiculously enormous wave of infections that might peak with half of everyone getting infected, and that causes peak hospitalizations anywhere from 0.5-2x the UK's previous peak from the alpha wave back in January (74k additional deaths on the high end, in the not-actually-possible-even-in-principle scenario).
Again, these scenarios aren't really possible (since no behaviour change is assumed), but they are useful for getting a sense of what Omicron could be like and the likely timings of things in the UK.
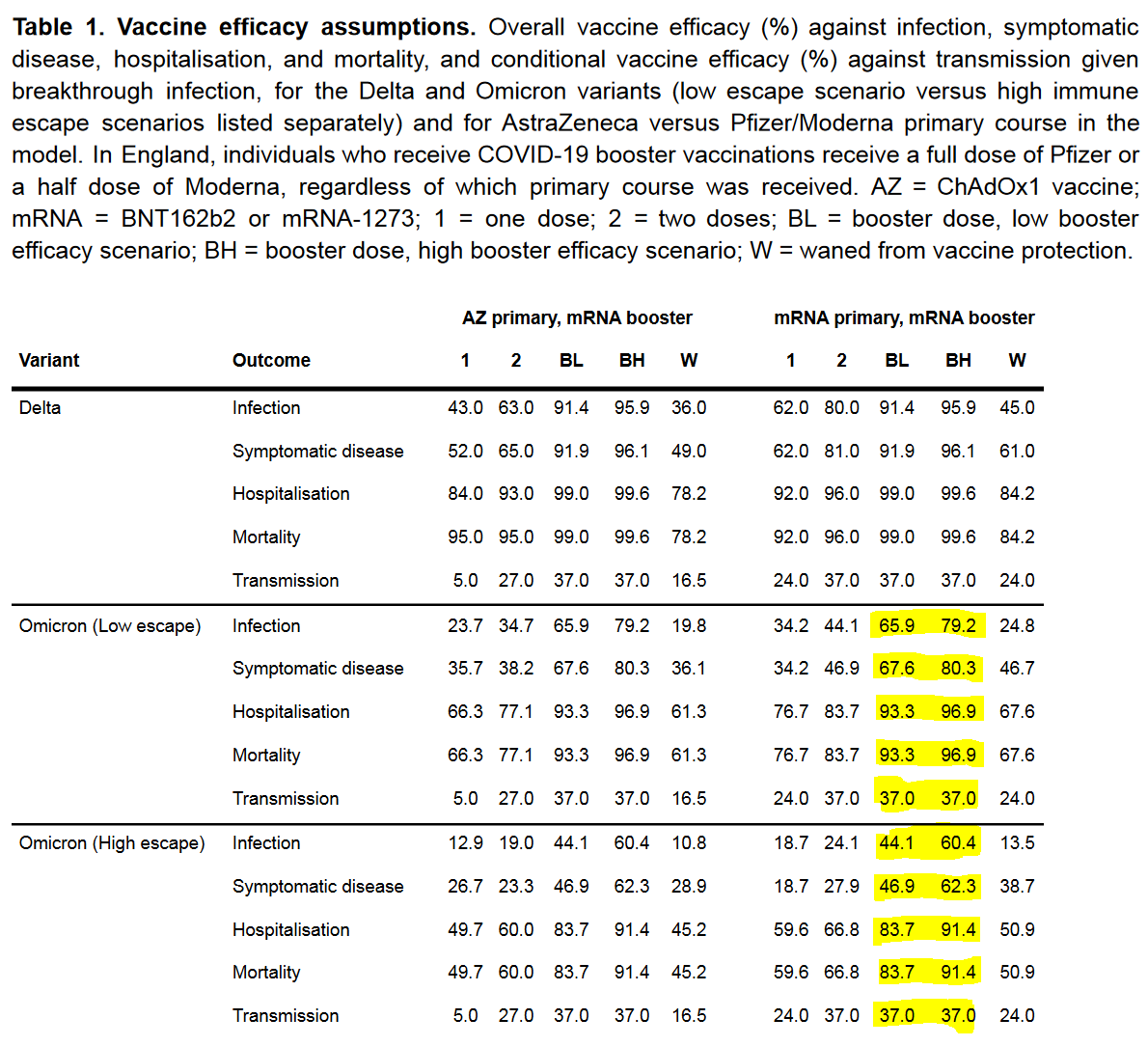
What's more useful for general readers is the paper's table of assumptions about vaccine efficacy vs Omicron - this was released just after results showed VE of Pfizer + Pfizer booster against symptomatic infection is 75%,
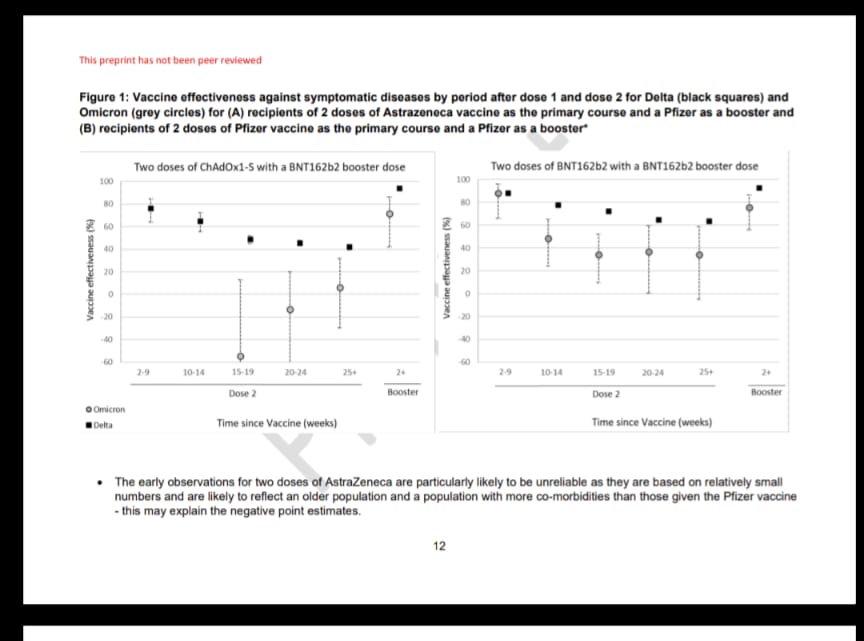
And here's the result from that Pfizer study:
I think the paper's results are based on trying to guesstimate just what properties are reasonable/vaguely consistent with what we've seen. The highlights in yellow are the ones that will matter in the long run for most readers - efficacy for 3-dose courses on low and high assumptions about Omicron immune escape and Booster efficacy.
The range for Symptomatic Illness efficacy is 46.9 - 80.3 %, though as I said the recent Pfizer study said the efficacy was 71.4% and 75.5% protection vs. symptomatic disease for people who received AZ and Pfizer primary courses, 2 weeks post their boosters. Don't know if that means we can bias ourselves towards the upper end of that range or not (1.9, 4.0, 5.0 times lower for the low, study result, high estimates of VE vs symptomatic infection).
The range for Hospitalization/mortality efficacy for a booster is 83.7-96.9%, or a 6.1 to 32.3 -fold reduction in mortality risk vs someone who isn't vaccinated against omicron. Again, adjust accordingly based on your age, sex and health vs the UK population average. Also note this isn't taking into account Omicron being intrinsically less severe, which it might well be.
Related, some guessing about which of the evasion scenarios we're in
The lower VE numbers here might be the plausible end of a range, or might just be the authors covering all possibilities, no matter how remote or absurd.
Fingers crossed, the apparently good efficacy of a booster that wasn't intended for anything like Omicron means that it's giving you generally broad-based immunity that will work going forward against whatever next crazy variant evolution throws at us.
I keep seeing extremely hard-to-judge theories thrown around, generally by suspicious types, about vaccine-granted antibodies being uniquely brittle and setting us up for the emergence of immune evasive variants - for example here. Dominic Cummings recently alluded to a similar idea - vaccines only targeting the spike protein (even though that was the best way to make a highly effective vaccine), means variant evolution can more easily evade vaccine antibodies than if they were broader.
AFAIK this is something that was considered during vaccine development (the reasoning was that there's fewer possible ways for the spike to change while keeping the covid virus still functioning, so targeting the spike would hopefully work against future variants), but which is in principle a problem for the future. Obvious caveat - you still get T-cell immunity no matter what's going on with the antibodies, which is the underlying reason why all the assumptions in the above table are high for severe disease immunity, and since we'll eventually end up in a scenario where most of the world has T-cell immunity to Covid from vaccines or infection, that will put a limit on the damage future waves can cause
It will be interesting to see how Evusheld fits into the vaccine mandate "ecosystem" especially in Europe where they make allowance for natural immunity despite having broader mandates.
Fantastic post, as always. Possible typos:
Is Omicron Going To Become the Primary Strain? Barring a new strain, 95% → 97%. ...
Chance that Omicron will displace Delta as most common strain: 95% → 96%.
and
We continue to have to [no] reason to suspect this, so I’m going to stop worrying about it.
The 97% was in case there was no other strain that comes in. So maybe the 96% is even taking into account another new strain? Or maybe it was just a typo.
Great work!
The thing is, at some point it does mean the virus is unstoppable, in the sense that no reasonable or worthwhile attempt to stop it has any chance of success, outside of at most protecting particular vulnerable groups and doing mitigation. If the baseline transmission is higher than Delta and it’s mostly ignoring vaccinations, what is your plan exactly? Lock down much harder than we did in 2020? Close the grocery stores?
Naïve calculation: if surgical masks blocked 75% of aerosols going out and coming in, and if all transmission were through aerosols, and if people wore these masks all the time, this could theoretically overcome R0 = 16 (because the transmission would be reduced a factor of four in both steps). Of course it will not work out this well, but then there are many other measures that can be taken in addition. So I think it would be technically feasible to keep it under control. But if it were to run quickly through most of the population, omicron would have to be much less severe than other variants to not overwhelm hospitals (without massive scale up of treatments).
Masks work by reducing the fraction of virus particles from an infected individual that get into the air, or the fraction in the air that get into the wearer. My understanding is that this isn't a direct multiplier on R0, it's a multiplier on how long (on average) you need to be around an infected person, or a concentration of aerosolized virus particles, before you've accumulated enough exposure to become infected yourself. Unmasked, with no immunity, the relevant exposure times (as measured early in the pandemic) were on the order of 15 minutes. Good masks for both parties would get you into the range of a few hours. Not sure how that changes with the newer and more infectious strains, but I assume the times are shorter. But basically, my take has been that if you're going to be around someone for more than a few hours (like your coworkers or classmates), then unless you're wearing N95 masks near-perfectly, it's unlikely they're going to accomplish much. Not literally nothing, but much less than they do for brief encounters.
It's hard to pin down a threshold of a specific time of exposure because it depends on the minimum infectious dose, which varies widely among people, at least for lots of diseases. Also, the rate of shedding varies widely based on the progression of the disease, whether the person is talking, how far away the person is, etc. Furthermore, the HVAC system causes additional variation. So I think when you add all these uncertainties, a 16 times reduction in emission/inhalation would correspond to very roughly a 16 times reduction in infection, but I would be very interested to see if someone has run the math on this.
A few key questions determine our fate. We are rapidly getting closer to the answers. That doesn’t mean we have the magnitudes of the answers. The magnitudes matter, and they matter a lot. It’s still a stronger understanding than even a few days ago. Next time will be stronger still.
My guess is that that Omicron for now is on a bi-weekly schedule, and the next update will likely be on Monday, but it is subject to what happens.
So here are some things that, for all practical purposes, we know.
Does Omicron Have Substantial Immune Escape Properties?
Yes. Just yes. Wenowdis. The laboratory results are in. The results from who is testing positive are in. This isn’t a question anymore. 95% → 99%+.
Here’s Pfizer’s press release from December 8. They note that there’s a large decline in vaccine effectiveness, but also observe that those who are boosted seem to still have enough protection, and that two doses seems sufficient to provide at least some protection. They don’t want to come out and say yet that there’s protection against severe disease with two doses, but there’s plenty of other evidence on that.
Here’s a thread of two threads with the preliminary data. It’s clear that vaccine effectiveness is down, but not as far down as we feared, and definitely not to zero.
Here’s a thread from Muge Cevik describing the results. Again, not great, but not as bad as expected.
We are seeing large declines in antibody effectiveness, with numbers like 25x or 41x fold decline being thrown about, most commonly 41x.
The key is to remember that this is not a game of ‘exactly enough’ antibodies or antibody effectiveness getting it done and less not getting it done. This is a case of things varying by multiple orders of magnitude. It sounds scary to hear a 41x fold decrease in effectiveness – that’s 98% – but in terms of whether and how much you get sick, that’s a lot less than 98% less effective.
Also, Bloom Lab has come up with a way to estimate potential immune escape properties in advance, as a function of mutations. Neat.
Here’s another intriguing data point: Google trends data in South Africa doesn’t reflect an increase in searches for loss of taste and smell. I wonder if this will hold up.
Does Vaccination or Delta Infection Still Protect Against Severe Disease And Death from Omicron?
Yes. Just yes. Wenowdis. The laboratory results are in. The results from South Africa are clear. People keep showing up positive for Omicron despite vaccinations and being fine. If this wasn’t true, we would know, or at least have reasons to be concerned, by now. 95%+.
And if this somehow isn’t true (not that I can reconcile that with the lab results), then the only way to explain the strain looking as mild as it is would be if it really was as mild as the raw numbers suggest, modulo age adjustments, which might be even better.
Is Omicron Going To Become the Primary Strain?
Yes. Just yes. Wenowdis. Only way it doesn’t happen that I can think of is that another strain comes out of nowhere and takes over first. This is happening. It’s when, not if. We know it has a lot of immune escape, and it spreads easily otherwise, so I can’t see how this doesn’t happen. Barring a new strain, 95% → 97%.
It’s probably going to happen fast.
We know it’s happening in the United Kingdom and Denmark because they are actually looking. Other places aren’t looking, so it isn’t as directly obvious, but this is happening. It’s certainly interesting that the USA and other countries aren’t finding more cases yet, which is why I’m not even higher, but my presumption is that other places simply aren’t checking. It’s not like we have a SGTF graph for California or Germany or wherever that doesn’t show a rise in deletions, we simply don’t have any data at all.
Here’s the UK statement from yesterday.
And here we go.
If it’s happening in one place, and happening this fast, why would anywhere else be any different, aside from exactly when things start taking off?
That’s a log-scale graph, and this is what we call a ‘straight line.’
As opposed to this graph, which has useful information but is formatted quite poorly, as a cumulative number that isn’t on a log scale:
This requires you to mentally do both conversions, and seems to show a somewhat slower growth rate that would still be plenty sufficient to get the job done.
Will We Have Omicron Boosters In Time To Matter?
Nope.
If it’s available by March, then by the time it’s actually used, the big wave that might actually get us will have come and gone. That doesn’t mean it will be worthless, I’m still happy they’re doing it, but if we don’t get there before February the biggest part of the value, the ability to avoid a possible crisis situation, will have been lost.
We still need to lobby the FDA, as hard as possible, to get them to approve these as soon as possible. Approval now, or an easier path to approval, could speed up manufacturing and distribution. And we need to get ready for rapid distribution. Better late than never. But I do expect this to be late.
It points out that the whole time that we had the ‘we can update if we need to’ idea, we were largely wrong. As a matter of science and engineering, it’s easy. As a matter of logistics, it’s damn near impossible when it actually matters. If you have enough time to deploy, deployment wasn’t that important.
Now here’s things we don’t know yet.
How Fast Will Omicron Become Dominant?
Not something we know but seemed logical to put it here.
Denmark and the United Kingdom are our only two robust data points for real world data.
I got some additional wastewater sources, but nothing that’s far enough along for this to show up in aside from Boston’s. Which got even higher so it’s not a blip, and it might be Omicron and might be Delta, either way it’s not good news.
We also have prediction markets at Polymarket. They say that it’s a coin flip whether Omicron will be 10% of USA cases by the end of the year, with a lot of variance. According to these markets, there’s an 88% chance it will be above 1%, and a 15% chance it will already be above 50%.
These numbers seem like they exist roughly in the same universe. We have ~10% to not break 1%, then ~40% chance to be between 1% and 10%, then ~35% chance to be between 10% and 50%, and 15% to be above 50%, due to a mix of how fast Omicron will grow and how low a base things started out at, plus some uncertainty in the method of estimation and thus grading. That kind of curve of probabilities is approximately how exponential growth under this kind of uncertainty should work.
One thing I found this week is that it is plausible that Denmark isn’t overestimating its Covid case count that much, maybe as little as 50% additional cases in 2020. That seems low to me, and presumably went up once vaccinations happened, but interesting.
For the United Kingdom, we have linear growth on a log scale, so no reason to not extrapolate it, while noting that what expands on a log scale is Omicron as a percent of Delta, not as a percent of all cases. If we simply extend the line on the graph above, we’d be looking at a takeover in the UK within two weeks, as this is a completely absurd growth rate. I’m not sure what’s going on with it being that large, but the UK government’s two to four week estimate seems reasonable here.
For Denmark, here’s what we know, these are cumulative numbers.
December 3: 18 omicron cases
December 5: 183 cases
December 6: 261 cases (+78)
December 7: 398 cases (+137)
December 8: 577 cases (+179)
I don’t have today’s number, but this seems clear enough. It’s a smaller growth rate, but we’re still talking about rapid growth, a doubling time of three days or less. The UK data is even scarier.
There’s no reason to assume these aren’t mostly random draws from the distribution of growth rates in Europe.
Given that, toy spreadsheet time. How many cases when causes us to his 10% of cases by end of year in the USA?
If we start with 15 cases on 11/21 (the 15 cases from the Anime Convention on that date that later tested positive), and nothing else, we’d get to 75k cases/day by end of year, so between 10% and 50%. So it seems like 10% by end of year should be a solid favorite at this point, something like 70%, and 50% by then should be very live and be something like 30%. One caveat is that this is detected tested cases rather than cases, and Omicron is milder in practice, so that could reduce the guess by a factor of several times. Given that, the markets don’t seem obviously crazy, but I still would rather buy than sell on all three.
January and February will be when the crisis comes if there is a crisis, or when the wave passes over us if the whole thing is so mild everything is fine. There are enough variables that it’s hard to pinpoint a date, wide error bars on this, but early February seems like the most likely time for the peak.
Is Omicron Importantly Milder Than Delta?
That’s the big question. If it is to a sufficient extent, maybe Omicron is even a blessing in disguise. If it isn’t, well, it doesn’t look good.
Last time I said the evidence was ambiguous. Here’s another attempted explanation of why it’s ambiguous.
I’ve seen this data point in a few places, including Your Local Epidemiologist, and it’s often referred to without the details, so it’s worth remembering what the details are.
We do have exponential growth in the number of ICU patients on a log scale:
But what else could possibly have happened with exponential growth in cases? Of course it’s going to look like this on a log scale, some percentage of cases end up in the ICU and the case numbers are growing like this on a log scale.
From December 7, article in Financial Times raises hope of potential milder severity for Omicron. The superficial signs certainly are quite promising, before we correct for who is getting Omicron. Yes, this feels different, and this is confirmation of that.
These ratios look stable, so the question is how much they need to be adjusted for the changes in the populations involved. Over time, it becomes less plausible that the population is continuing to stay especially young. That goes double if the cases are mostly ‘people who came to the hospital for other reasons and happened to have Covid’ since that should be a relatively older population that’s in many ways holding constant.
The problem is that all of this continues to not answer the question of what happens when you adjust for the different populations in the different waves. I’ve yet to see a real attempt to do this properly. It’s hard.
The fundamental clash, where cases are milder but that doesn’t mean we know Omicron is milder due to different populations, makes this easy to misinterpret. Here’s Dr. Fauci talking about the situation:
That seems exactly right, and an attempt at clear and honest communication, and here’s the headline of the article.
Yeah, that’s… not what you’re quoting him as saying. At all. And it’s quite a big difference.
Pfizer CEO comes out and says yes, billions will get infected by Omicron, and again says it might be milder but we don’t know. He raises the concern of further mutations from all those infections.
He ends on a very optimistic note, or one might call it a rallying cry.
The question will not be whether normality will be the correct response. The question will be whether we are allowed to have normality, and how much we will fight for it.
Overall the news here is promising, but nothing like conclusive, and my probabilities didn’t shift much. No one’s doing the comparisons that would tell us the answer, not yet.
WHO Delenda Est
Ah yes, something else we know.
Kai thread covering a WHO presser. Notice how they manage to say a bunch of true things but avoid making any inferences, useful statements, probability or magnitude assessments, or calls for actions other than information gathering and what they were already calling for.
The whole thing is so perfectly on the nose and a master class in that movie scene where the expert goes on and is actually optimizing for uselessness. Observe these pieces of poetry, if that is relevant to your interests, if not skip the section.
To start off with, let’s be clear, says Tedros, we know nothing.
Note that complacency will cost lives, but that’s no excuse for drawing conclusions from limited information or otherwise making decisions under uncertainty. That would be reckless and irresponsible.
I suggest a Saturday Night Live debate between Dr. Tedros, who I suggest be played by special guest Don Cheadle, and Dr. Weknowdis. The topic should be: Resolved: We Know This? Or we don’t know this?
Seriously, you must act now, but also you can’t think you know anything when deciding how to act.
What the hell, doctor, do you want these people to do?
Notice that the first concrete action he mentions is to stop doing the one thing people tried doing. Still, I think I now agree on this as a concrete question, although it’s tricky, since if you have ten times as many cases as before, but so does South Africa, does lifting the ban make sense? I think the math basically says yes around now it no longer matters, but I haven’t done the math properly.
We must act now, except we must not act now. Also, that one useful thing your government is begging, pleading, and increasingly outright forcing you to do? Yeah, we’re still strongly opposed to that, despite Omicron.
Kai got to ask a question, and it was a useful one, especially in light of the answers to previous questions, great choice.
The thing is, at some point it does mean the virus is unstoppable, in the sense that no reasonable or worthwhile attempt to stop it has any chance of success, outside of at most protecting particular vulnerable groups and doing mitigation. If the baseline transmission is higher than Delta and it’s mostly ignoring vaccinations, what is your plan exactly? Lock down much harder than we did in 2020? Close the grocery stores?
Approve or deploy new measures quickly? Nope, not interested. Double down on the same stuff that destroys life and can’t possibly work? Yep, that’s the ticket. Insert meme here.
Except, you know, don’t get vaccinated if it’s a booster, continues to be WHO’s position, if I’m reading this thread correctly. I don’t understand how they intend to protect the health care system.
There’s a few more but I’ll cut it off here. At this point it seems like it’s descending into health-expert-talk-soup. Get vaccinated, except for most people who could get vaccinated, don’t. This is a global problem and that means doing, I don’t even know what at this point, but you can’t fight it while others aren’t fighting it, so do they want people to stop or something? I mean, yes, they seem to want this? We have to reduce transmission, but our focus is on hospitalization, severe disease and death?
Also, as for vaccinations, you know what works, however much one might still not want to use them? Vaccine mandates. So guess what the WHO is warning people against right now.
This is delay in the name of formality and in the name of looking like one has gone through proper procedure and signaled an appropriate dedication to avoiding blame, rather than any sense of urgency or attempt to win the game. It’s about whether you can point to having exhausted other options, not about whether the benefits of a mandate were worth the cost.
It’s not like there’s a big chance that ‘reach out to communities’ will magically solve your problem here. Pretty sure we’ve run enough of that experiment to know it might help but definitely won’t be a full solution. Either the mandates are worth the price, so go ahead and do them, or they’re not, and you shouldn’t wait until later and then do them anyway after their benefits are much reduced. That doesn’t actually accomplish anything besides blame avoidance.
If you’re against boosters and you’re against vaccine mandates then how would you describe that position? What if they also opposed travel restrictions, and opposed quarantines, and didn’t mention getting people tested quickly or getting them treatments?
Also notice there is not a single mention anywhere here of any treatment options whatsoever. Have you heard of Paxlovid? Fluvoxamine? Monoclonal antibodies? Nope, nothing, not a thing. The word ‘test’ appears once, on a country level in the context of data gathering, never in terms of patient treatment or expanding capacity or speed.
If you wanted things to be maximally bad through a combination of disease and costly efforts that disrupted our lives, what would you say differently?
Notice how this isn’t well-considered strategic thoughts with different world models, and it isn’t mustache-twirling villainy, it’s a jumbled mess of nonsensical calls for Sacrifices to the Gods, a broken robot repeating the same lines it’s been programmed to say without checking to see if that would accomplish anything or form a coherent model.
Summary Threads and Articles
Sarah Zhang at The Atlantic gives an overview that is effectively a reasonably good basic ‘exponential growth of even a relatively mild thing is very bad news because math’ explainer. No new information.
Thread wondering about first versus second generation lineages, and how additionally worried we should be for future variants.
Your local epidemiologist weighs in on a variety of topics. Good summary of some things we know, but high reluctance to be confident in or extrapolate to the natural conclusions.
Natalie Dean uses sketches to explain why the strain that immune evades appears milder.
Other Notes
Israel is softening its quarantine to allow grandparents and parents in for the birth of children. I consider this a sufficiently large leak that I don’t see the point of keeping the quarantine. Either play to win the game, or don’t.
Probability Updates
This includes repeats of stuff above, so it’s all in one place.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 65% → 75%.
A full 100% still feels like a lot, variants start out under weird circumstances and with advantages, and different places are different, but the UK data seems very clear and Denmark’s is suggestive as well.
Chance that Omicron will displace Delta as most common strain: 95% → 96%.
You never know, a miracle might occur?
Chance that Omicron is importantly more virulent than Delta: 5% → 4%.
Chance that Omicron is importantly less virulent than Delta: 50% → 55%.
It does seem like chance of more virulent continues to decline, but the chance of less virulent hasn’t changed much because we’re basically in the same spot as before. It does seem like there’s more consensus that milder is likely, so a small adjustment I guess.
Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 95% → 99% (and I’ll stop listing this unless that changes).
Will the CDC label Omicron a variant of high concern before 2022? 13% → 12%.
I don’t see much eagerness in the CDC to do this so I am fine respecting the market price.
Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 2.5% → 2% (and I’ll stop listing this unless it goes above 2%).
We keep getting strong evidence this isn’t true.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 60%.
Announcements for boosters within three months seem commonplace, although still with a lot of ‘if necessary’ still attached to everything and timelines that can slip. This does now seem like the baseline thing to happen, but still not all that confident.
Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 3% → 2.5% (and I’ll stop listing this unless it goes up).
We continue to have to reason to suspect this, so I’m going to stop worrying about it.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 17% → 25% (edit later that day) → 25%
A lot of this is the vibe of what I’m seeing, and how likely we are to react in various ways if the hospitals do look like they’re on the verge of being overwhelmed. Would we actually try this?
Will Omicron be >1% of all cases by the end of the year? 93% → 94%.
The UK and Denmark data seem to emphasize this but I did expect to see larger growth in detected cases elsewhere, and there’s still a long way to go, and the prediction market hasn’t gone too far towards 100% although it’s known that prediction markets are in general too low once numbers get this high.